This research aims to analyze the deployment of lean practices and resilience capabilities within the healthcare supply chain across different disruptive scenarios. The study addresses the gap in how different tier levels of the healthcare supply chain integrate lean and resilience.
Employing a case study approach, the research evaluated four Italian organizations (two healthcare providers, one pharmaceutical distributor and one pharmaceutical producer) representing the three main tier levels of the healthcare supply chain. The methodology involved a questionnaire assessing the adoption of specific lean practices and resilience capabilities, followed by a scenario analysis by experts used to identify critical practices and capabilities across different disruptive scenarios.
This research systematically identified critical lean practices and resilience capabilities that are underutilized at various tier levels within the healthcare supply chain, highlighting significant opportunities for theoretical advancement in operational efficiency and system robustness during disruptions. Additionally, the study introduced a novel methodological approach to evaluate the effectiveness of lean and resilience practices across different disruptive scenarios, thereby enriching the theoretical framework for crisis management within healthcare operations. Finally, we emphasized the crucial roles of just-in-time and anticipation capability in bolstering the performance of all the healthcare supply chain.
The study contributes to the fields of supply chain management and healthcare by systematically identifying and classifying the importance of lean practices and resilience capabilities in managing disruptions. Additionally, the potential for cross-tier collaboration and knowledge sharing to enhance overall supply chain resilience is highlighted.
1. Introduction
Lean supply chain consists of organizations directly linked by upstream and downstream flows of goods, services and information that work together to reduce costs and waste by fulfilling the essential needs of customers (Núñez-Merino et al., 2020). Within various industry sectors, the healthcare supply chain emerges as a pivotal application of lean, given its paramount role in safeguarding and enhancing human lives (Khorasani et al., 2020). However, some disruptive events, such as COVID-19 outbreak, on healthcare operations have raised many questions about the lean management applicability and capability of healthcare to respond to critical events (Ivanov, 2021). These concerns stem from potential operational adjustments linked to the adoption of lean practices, including significant reductions in inventory levels and a noticeable lack of redundancy, which can affect the resilience of the supply chain (Ruiz-Benítez et al., 2018).
Contrastingly, some scholars highlighted a significant synergy between lean and resilience in the healthcare supply chain. Leite (2022) affirmed the positive impact of lean practices on resilience during disruptive events, emphasizing their crucial role in supporting healthcare organizations in critical situations. Additionally, Kuiper et al. (2022) argued that lean methodologies can alter underlying trade-offs, making healthcare continuity more robust against catastrophic events, and thereby increasing resilience. In line with this, Birkie (2016) reported a positive synergy between resilience and lean practices when confronted with disruptions of varying natures and intensities. As a result, the combined effect of lean and resilience seems to be complementary, surpassing the benefits of each approach individually and resulting in enhanced operational performance.
Despite the presence of evidence supporting a positive relationship between lean management and resilience, the literature reveals a notable scarcity of studies specifically addressing their combined application within the healthcare supply chain (Habibi Rad et al., 2021). This is especially evident in works that dissect how these practices are implemented across different tier levels of the healthcare supply chain (Alemsan et al., 2022). Furthermore, the literature lacks comprehensive exploration of how lean management and resilience are addressed in the face of disruptive scenarios in healthcare sector, such as supply chain crises (Touriki et al., 2021). Based on these arguments, a research gap is identified with respect to the combined deployment of lean practices and resilience capabilities in the healthcare supply chain, raising the following research question (RQ):
How does the deployment of lean practices and resilience capabilities vary within the healthcare supply chain across different disruptive scenarios?
To answer this RQ, this study analyzed the deployment of lean practices and resilience capabilities within the healthcare supply chain across different disruptive scenarios. For that, multiple case studies were conducted involving four organizations from the Italian healthcare supply chain, which belonged to three different tier levels. This study presents theoretical and practical contributions. Theoretically, the study advances the understanding of the interaction between lean practices and resilience capabilities within the healthcare supply chain, particularly during disruptions. Also, the study adds to the literature by examining the implementation of these practices and capabilities across different tier levels, providing insights into their synergistic potential. Practically, this study provides valuable information to help formulate strategies that guide managers towards more efficient and resilient supply chain operations. Furthermore, the study enables a systemic view of the healthcare supply chain, encouraging an understanding of how each organization contributes to the whole, rather than focusing solely on individual organizational performance.
2. Background
2.1 Lean and resilience in the healthcare supply chain
The discourse surrounding resilience in the healthcare supply chain has gained significant traction, especially in light of the COVID-19 pandemic (Spieske et al., 2022). Among the myriad strategies for enhancing resilience in the healthcare supply chain, Rehman and Ali (2022) propose that Industry 4.0, multiple sourcing, risk awareness, agility and global diversification of suppliers, markets and operations are the most significant strategies to enhance healthcare resilience. Following this perspective, Furstenau et al. (2022) expand on the adoption of digital technologies such as big data analytics, predictive health data analysis and remote monitoring of inventories to improve resilience in the healthcare supply chain.
Concurrently, lean practices have been recognized for their potential to bolster supply chain resilience through improved coordination, communication, capacity building and awareness (Hussain et al., 2022). In the healthcare supply chain context, Yilmaz et al. (2023) introduce an optimization-based methodology utilizing lean practices and emphasize the importance of employing a pre-disruption strategy via the proposed methodology to design a resilient supply chain to be prepared for disruptions. Also, Alemsan and Tortorella (2022) confirmed the correlation between resilience and lean and the mediating role of resilience development in the association between lean principles adoption and operational performance. In addition, Rosso and Saurin (2018) argued that the joint use of lean practices can effectively address the efficiency-thoroughness trade-off in complex systems, thereby enhancing resilience.
Furthermore, research has recently stared to explore the application of lean management and resilience at different healthcare supply chain tier levels. For example, at the upstream level, Saraji et al. (2023) introduced a framework for assessing pharmaceutical companies’ performance in lean, agile, resilience and green adoption, emphasizing design for manufacturing and strong communication with suppliers as critical challenges. On the downstream level of the healthcare supply chain, Samieinasab et al. (2022) proposed a comprehensive framework for evaluating and enhancing clinical department performance by integrating resilience and lean principles and they find the need for a balanced approach, as clinics demonstrating excellent resilience performance may lack lean performance, and vice versa.
2.2 Supply chain disruptions
Systems with many elements as supply chains can be vulnerable to nonlinear interactions as disruptions and causing severe impacts (Pettit et al., 2013). Supply chain disruptions can be defined by unplanned and unanticipated events that disrupt the normal flow of goods and materials within a supply chain (Macdonald and Corsi, 2013). The disruption process starts with its identification and understanding, progresses through recovery efforts and concludes with restoration and subsequent redesign measures to enhance the process (Messina et al., 2020). The decisions made by supply chain managers greatly influence the speed and efficacy of the recovery process (Shekarian and Mellat Parast, 2021). Therefore, effective management of disruptions is crucial for maintaining the resilience and smooth operation of supply chain systems in the face of unexpected events (Birkie et al., 2017).
Disruptions can be classified based on their origin, such as internal and external disruptions. For instance, internal disruptions stem from failures or resource issues within a company, while external disruptions result from events beyond the supply chain, including natural disasters, political instability, terrorism and global financial crises (Park et al., 2016). Furthermore, disruptions can also be categorized by their causes, including natural, technological, economic and political disruptions (Peck, 2005). Additionally, disruptions can be classified by their impact on the supply chain, encompassing issues like raw material availability, production interruptions, delivery delays, quality problems and supply chain failures (Macdonald and Corsi, 2013).
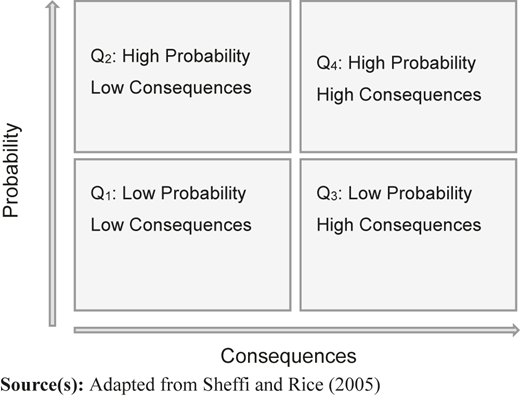
Another possible classification of disruptions in supply chains is based on their occurrence probability and consequences. Sheffi and Rice (2005) proposed a matrix that categorizes disruptions into four vulnerability quadrants as shown in Figure 1. Low probability and low consequence events could include equipment failures, sporadic supplier issues, small security incidents and minor deviations in product quality (Quadrant 1). High probability but low consequence events could include minor logistical delays, temporary shortages of non-critical medical supplies and brief communication disruptions (Quadrant 2). Low probability but high consequence events, such as severe natural disasters, pandemics, terrorist attacks and major recalls of medical products, are rare but can severely affect the system (Quadrant 3). High probability and high consequence can include events include worker strikes, IT system failures, delays in the delivery of critical medications and supply chain disruptions for essential medical equipment (Quadrant 4).
Considering the classifications of supply chain disruptions, healthcare systems emerge as particularly vulnerable to disruptive events, with severe implications for service performance (Samieinasab et al., 2022). For instance, a halt in pharmaceutical production due to regulatory changes or geopolitical tensions can quickly lead to shortages of essential medications, compelling healthcare providers to seek alternative treatments, potentially at higher costs and with less efficacy (Roscoe et al., 2020). Similarly, natural disasters can disrupt the logistics of medical supply delivery, leading to critical delays in treatments and surgeries (Razavi et al., 2021). Additionally, strikes or labor disputes in key logistics sectors can interrupt the flow of critical supplies, leading to operational bottlenecks and compromised patient care (Youssef et al., 2021).
Therefore, a comprehensive analysis of how lean practices and resilience capabilities perform under various disruptive scenarios remains lacking in the literature, highlighting a significant gap that this study aims to address.
3. Method
To achieve the objective of this study, a case study was conducted. According to Yin (2018), case study is a research strategy that allows an in-depth and detailed investigation of a phenomenon in its natural context. The study consisted of four steps: (1) defining the assessment criteria for lean and resilience; (2) selecting the healthcare supply chain organizations to be evaluated (3) assessing the importance level of each lean practice and each resilience capability across different disruptive scenarios and (4) determining the most critical lean practices and resilience capabilities.
3.1 Defining the assessment criteria for lean and resilience
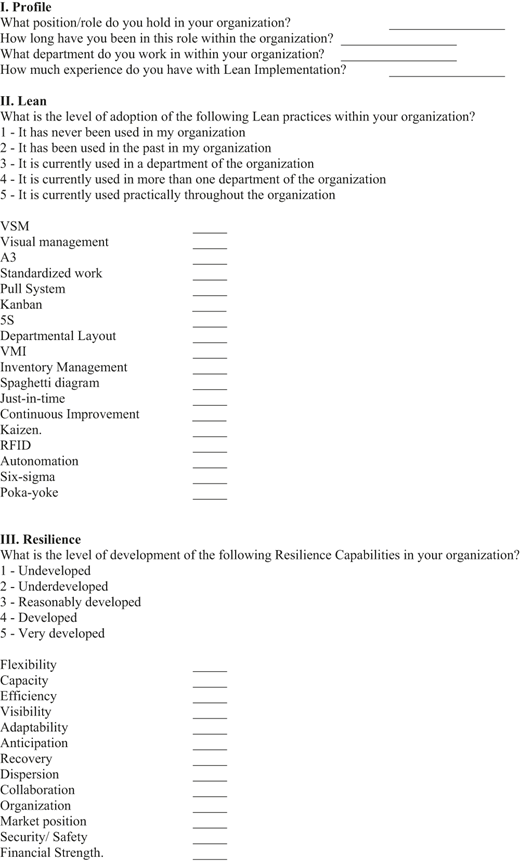
A questionnaire (see Appendix) was prepared to assess the level of adoption of lean practices and resilience capabilities within the organizations. Both the selected lean practices and resilience capabilities were based on the framework developed by Alemsan et al. (2022), which was developed after an extensive literature review. For lean adoption assessment, the questionnaire included lean practices such as value stream mapping (VSM), visual management and A3. Regarding resilience adoption assessment, the questionnaire comprised resilience capabilities such as visibility, adaptability and anticipation. Participants were asked to rate the level of adoption for each lean practice and resilience capability on a Likert scale from 1 (“it has never been used in my organization”) to 5 (“it is fully used in my organization”). We obtained a Cronbach’s alpha of 0.876 and 0.823 for lean practices and resilience capabilities, respectively, indicating the high reliability of our instrument.
3.2 Selecting the healthcare supply chain organizations to be evaluated
To select the organizations that could provide the proper context to develop our case study, a few criteria were established. First, regarding the healthcare supply chain tiers, Moons et al. (2019) defined three main levels of the healthcare supply chain: producers (e.g. medical device manufacturers, pharmaceutical companies, etc.), purchasers (e.g. purchasing organizations, distributors, etc.) and healthcare providers (e.g. hospitals, clinics). The chosen organizations should represent these three tier levels of the healthcare supply chain. Second, organizations should present prior experience with lean implementation, and their interviewed employees should have actively participated in lean projects. We also sought for a diverse and multidisciplinary group of participants, including individuals from various sectors and roles, such as medical directors, nursing coordinators and planning managers. Third, to ensure coherence in our unit of analysis, the selected organizations should belong to the same healthcare supply chain. Due to its inherent relevance, we chose medicines as the stream to be analyzed throughout the healthcare supply chain. The choice of focusing on the medicines flow was motivated by several reasons. Firstly, medicines flow plays a critical role in the healthcare supply chain as it directly impacts the quality of patient care (Iqbal et al., 2017). Also, the availability, quality and safety of medicines are fundamental for ensuring the success of treatments (Khorasani et al., 2020). Moreover, the medicines flow significantly influences healthcare costs, encompassing expenses related to the drugs themselves, as well as transportation, storage and inventory management (D’Ambrosio et al., 2020). Finally, the complexity of medicines flow is high due to the wide variety of medications and large number of stakeholders, from manufacturers to patients (Merkuryeva et al., 2019).
3.3 Assessing the importance level of each lean practice and each resilience capability across different disruptive scenarios
Based on the work of Sheffi and Rice (2005), four disruption scenarios were identified as described in Section 5.2.2 of this article. The aim of this step was to assess how each lean practice and resilience capability stood up against various disruptive scenarios. Participants evaluated and assigned a level of importance, ranging from 1 (least important) to 5 (most important), to each identified lean practice and resilience capability within the context of these scenarios. To ensure the highest level of expertise, eight academics who actively worked and researched in the investigated phenomenon were invited to share their opinions. That helped secure in-depth and legitim insights related to the topic. To achieve a balanced and representative analysis, the median of the assigned importance levels was calculated for each practice and capability.
3.4 Determining the most critical lean practices and resilience capabilities
From the results of the questionnaire about the adoption level, the median of the lean practices values was identified. Subsequently, the gap for a full adoption was calculated by subtracting the median from 5 (Equation 1), aiming to quantify the gap between the current adoption level and the ideal state. The adoption gap highlighted the potential for improvement in the adoption of lean practices and resilience capabilities. The adoption gap was then multiplied by the importance level of each lean practice generating the criticality factor (Equation 2). This step generated four columns of data for each organization, one for each disruptive scenario, which was then be standardized (Equation 3). Through standardization, the most critical items for each organization and scenario were identified, specifically those items with values greater than 1 (Tortorella and Fogliatto, 2014). These items were deemed critical because, despite their recognized importance, they were not sufficiently adopted within the organization, indicating a significant potential for operational improvement. The equations involving resilience capabilities were similar and they are showed in Equations (4), (5) and (6).
Where:
Where:
4. Results
4.1 Case study
In this section, the results are presented. Firstly, Italy was the country chosen for the application of the case studies due to several reasons. Italy was a country hard hit by the COVID-19 pandemic, which brought significant challenges to its healthcare supply chain (Remuzzi and Remuzzi, 2020). The Italian response to the crisis, including reorganizing its healthcare supply chain, provided valuable insights to crisis management, resilience and innovation under extreme disruptive events (Torri et al., 2020). In addition, Italy has an aging population (Spaccattini et al., 2022), which poses unique challenges for healthcare supply chain management. The case study focused on the medicine flow sector, where Italy plays a significant role and is considered one of the main players in the European pharmaceutical industry (Musazzi et al., 2020). The Italian pharmaceutical industry is second to the German one, as it represented 26% of total production and 19% of the market in the five biggest European Union countries (Toma, 2020). Also, in recent years Italian pharmaceutical exports grew by 56% compared to the European average of 33% (Toma, 2020). Therefore, the case study on the flow of medicines in Italy could offer valuable insights to the study.
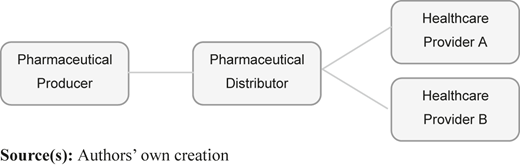
The supply chain structure under study was composed of four organizations: two healthcare providers, a pharmaceutical distributor and a pharmaceutical producer, as depicted in Figure 2.
The Healthcare Provider A was the first hospital in Italy to effectively implement lean practices in the healthcare industry, receiving an award in recognition of its achievement. This award is organized by a consortium of prestigious Italian healthcare and educational organizations as the Italian Federation of Hospital Companies. Furthermore, the hospital boasts several noteworthy lean projects across the entire facility, with some being honored for their excellence. To ensure seamless implementation of the lean approach, the hospital has established a multidisciplinary lean team. As part of its commitment to continuous improvement, the hospital offers its employees courses on lean management, aimed at enhancing their knowledge and skills.
The Healthcare Provider B has a different structure. The company is responsible for providing medical care and health services to a population and it is made up of 13 operating units. The healthcare company won a Lean Healthcare Award for the best lean project idea under implementation. In addition, this hospital was nationally recognized as one of the most advanced hospitals in lean healthcare.
The selected Pharmaceutical Distributor maintains a strong connection with both healthcare providers. In addition to handling procurement, warehousing and distribution logistics, this pharmaceutical distributor is also responsible for managing tender procedures and implementing advanced information and communication technologies for hospitals.
The organization selected to represent the Pharmaceutical Producer is one of the leading firms in Italy, with significant revenue and a long-standing commitment to lean practices, offering certification programs like Lean Six Sigma to its employees.
4.2 Data collection and criticality of lean practices and resilience capabilities
Following the selection of organizations, a total of 100 responses were collected from employees of these four organizations. The data collection occurred between April and July 2023. The methods of communication included LinkedIn, email and coordination with a designated representative from each organization, which facilitated internal dissemination of the questionnaire. The respondents’ data is included in Table 1.
From the results of the questionnaire, Table 2 and Table 3 provide the data derived from the equations detailed in the Method Section. In gray, there are the most critical lean practices and resilience capabilities for each scenario of disruption, identifying those with a standardized criticality factor (ZC) exceeding 1. Statistically, a ZC greater than 1 signifies that the associated value is more than one standard deviation above the dataset’s mean, marking the practice or capability as significantly critical. Such a ZC indicates the imperative areas where enhancing adoption could result in substantial improvements, given the pre-established importance of these items.
Table 2 allows the identification of the most critical lean practices across four organizations and four disruptive scenarios. Eleven different lean practices were identified as critical, such as JIT, lean six-sigma and poka-yoke, indicating areas where improvements could yield substantial operational benefits. Additionally, Table 3 shows the criticality levels for resilience capabilities. The analysis reveals that only six of these thirteen capabilities are considered critical, distributed across the four organizations and four disruptive scenarios, highlighting specific areas where improvements are necessary to enhance organizational resilience. The identified critical resilience capabilities are anticipation, recovery, adaptability, organization, financial strength and collaboration.
Table 4 improves the visibility of the data by presenting the most critical lean practices and resilience capabilities for each organization and each disruptive scenario in a consolidated manner. This table provides a clearer overview and facilitates easier comparison across different scenarios and organizations.
4.3 Within case analysis
4.3.1 Pharmaceutical Producer
The identification of poka-yoke, A3 and JIT as critical practices across all scenarios for the Pharmaceutical Producer highlights the need to bolster quality control, enhance problem-solving capabilities and improve operational efficiency. The underutilization of poka-yoke practice might result from a lack of comprehensive training or understanding of its error-prevention benefits in a sector where errors can have significant implications. The rarity of A3 practice might reflect an organizational environment not fully embracing structured problem-solving or a deficiency in skills necessary for facilitating these processes effectively. Lastly, the limited adoption of JIT practice suggests the difficulty in aligning its principles of lean inventory with the unpredictable demands and strict regulations of pharmaceutical production.
Regarding resilience, in scenarios of high probability, no resilience capability was considered critical. On the other hand, The critical nature of anticipation and recovery capabilities in scenarios of low probability could be attributed to a general lack of preparedness for rare events. Organizations often focus on mitigating risks they frequently encounter, leading to well-established responses for common scenarios. However, rare events can catch these organizations off guard, necessitating a broader range of capabilities to effectively respond.
4.3.2 Pharmaceutical Distributor
The identification of JIT as a critical practice within a Pharmaceutical Distributor highlights a significant operational gap. This shortfall points to the necessity of creating a JIT culture more deeply within the organization to ensure timely medication delivery, crucial in the healthcare sector. The identification of A3 as critical in high probability scenarios underscores the need for structured problem-solving approaches in environments where disruptions are frequent. By promoting in-depth analysis of problem roots and encouraging evidence-based solutions, A3 equips organizations with the ability to effectively address and prevent the causes of recurring disruptions (De Barros et al., 2021). Additionally, the presence of the 5S practice in the last three disruption scenarios highlights its crucial yet underdeveloped role in pharmaceutical distributor operations. 5S is vital for ensuring efficient, error-free distribution of medications, directly affecting patient care (Costa et al., 2017) and its current underutilization, suggesting an opportunity to enhance their operational practices and maintain a safer and more productive work environment.
Regarding resilience, the criticality of anticipation capability in all scenarios underlines the foundational importance of forward-looking strategies to mitigate potential disruptions. It implies a strategic gap in the organization’s current preparedness efforts, highlighting an area for immediate improvement. The mention of Organization capability in the first scenario points towards the need for well-defined processes, teamwork, training and a structured approach to manage and recover from minor disruptions efficiently. This capability is important for maintaining order and ensuring that operations can continue smoothly with minimal impact, even when disruptions are deemed unlikely and of low impact (Pettit et al., 2013). The introduction of adaptability capability in the scenario with both high consequence and high probability highlights the need of the organization to be dynamically responsive in the face of significant and likely disruptions.
4.3.3 Healthcare Provider A
The analysis of lean practices and resilience capabilities across various disruptive scenarios reveals key insights for Healthcare Provider A as the consistency of lean six-sigma and poka-yoke practices emerging in all scenarios. The analysis suggests that, although these practices are highly valued for quality control strategies and error prevention, there are opportunities to broaden their adoption and amplify their benefits. This underutilization can often be attributed to several key factors. First, the complexity and perceived rigidity of implementing lean six-sigma and poka-yoke practices might deter organizations, particularly those with limited exposure to systematic quality improvement practices (Samanta and Gurumurthy, 2023). Also, the lack of awareness about the existence of lean six-sigma and poka-yoke practices could significantly contribute to their underutilization (Kumar and Steinebach, 2008). This gap in knowledge prevents organizations from even considering these practices as part of their quality control and error prevention strategies. Furthermore, the shortage of skilled practitioners who can lead such initiatives and mentor staff is another critical barrier, complicating the deployment of these methodologies in settings that could benefit from them the most (Vinod et al., 2015).
Also, the kaizen practice is prominent in low consequence scenarios independent of probability. Despite its high valuation, kaizen underutilization points to a critical need for broader implementation, exacerbated by its limited recognition and understanding among hospital staff and management (Shatrov et al., 2021). Without sufficient knowledge or training, the full spectrum of kaizen benefits might not be appreciated, which could result in reluctance to adopt the practice (Hasle et al., 2016). Also, the upfront investment needed for training and process reengineering to implement Kaizen effectively can act as an obstacle, especially in hospitals where resources are limited (Harry, 2020).
For high consequence disruptive scenarios, VMI, RFID and autonomation are deemed critical. These practices are pivotal for ensuring that hospitals can maintain operational stability and continue to provide essential services during and after disruptions. Despite their significant potential for mitigating risks associated with such events, several factors contribute to their underutilization. First, the initial investment required for these technologies can be substantial, encompassing not only the cost of the technologies themselves but also the expense of integrating them into existing hospital operations (Dachyar and Yolanda, 2020). The integration of these practices into the hospital existing systems and processes involves a considerable degree of complexity. It requires a seamless blend of these technologies with current operational workflows, which can be challenging without the requisite technical expertise and IT infrastructure (Afoakwah et al., 2023).
Regarding resilience capabilities, in the first scenario with low probability and low consequence, no capability was considered critical, indicating that the practices deemed most important are already widely adopted. The consistent presence of anticipation and recovery capabilities in the last three scenarios suggests their relevance and increasing importance in more complex and challenging situations. In high probability but low consequence scenarios, the ability to foresee and swiftly respond to a succession of minor disruptions is crucial for maintaining uninterrupted operations and ensuring that such events do not cumulatively degrade the system resilience (Safa et al., 2021). Conversely, in scenarios marked by low probability and high consequence, the criticality of anticipation and recovery capabilities reflects the imperative to be well-prepared for rare but potentially devastating events (Sawyerr and Harrison, 2023). The analysis shows a clear need for better preparation for disruptions and quicker recovery after they happen. It suggests organization should both look ahead to spot possible disruptions through risk assessments and also have clear recovery plans ready for getting back to normal quickly once a disruption occurs (Senna et al., 2023).
4.3.4 Healthcare Provider B
For Healthcare Provider B, an analysis uncovers the consistent underutilized roles of kanban and JIT practices for all scenarios. This underutilization likely stems from a lack of knowledge within the Healthcare Provider B about how these lean practices, which complement each other, can be effectively integrated into healthcare settings. JIT focuses on cutting inventory and lead times, while kanban enhances workflow efficiency, providing a robust method for hospitals to manage disruptions (Siddiqui, 2022). The insufficient adoption of these methodologies suggests a gap in understanding their combined potential to streamline operations, reduce waste and ensure the availability of essential supplies precisely when needed, thereby maintaining continuity of care (Khorasani et al., 2020).
Regarding resilience capabilities, in all four disruption scenarios, the anticipation capability is consistently identified as both critical and underdeveloped within the healthcare system, indicating a systemic shortfall in the Healthcare Provider ability to foresee and prepare for potential disruptions. This gap, present across scenarios of varying probability and consequence, highlights a pressing need for the healthcare provider to enhance its predictive planning and risk assessment capabilities. The lack of anticipation capability suggests an organizational focus that may lean more towards reactive rather than proactive strategies, undermining the systems resilience and its ability to maintain operational stability and continuous patient care in the face of disruptions (Agostini et al., 2023).
5. Discussion
In a broad analysis, it becomes apparent that JIT practice, with the exception of Healthcare Provider A which already exhibits high adoption, is significantly underutilized across the organizations within the healthcare supply chain. This disparity raises questions about the scalability and adaptability of JIT in environments characterized by unpredictable demands (Hundal et al., 2021). By looking at previous literature, Kaswan et al. (2022) highlight that failures in JIT execution often stem from a lack of insights into the enablers of successful implementation such as top management support, teamwork and real-time information sharing. Similarly, Balkhi et al. (2022) identify that during the COVID-19 pandemic, shortages were exacerbated by JIT systems failing to meet unexpectedly high demands. This underlines the critical need for accurate demand forecasting. Furthermore, precise estimations of consumption patterns are essential, requiring robust tools to calculate and predict which items are at higher risk of shortage and which are not (Balkhi et al., 2022). In the same way, Siddiqui (2022) cite some disadvantages of JIT as the limited room for error due to minimal stock levels maintained for re-working faulty products, and the highly vulnerability to disruptions from natural disasters. In sum, JIT just works properly when the organization has reliable and accurate demand forecasting and works with reliable suppliers (Balkhi et al., 2022). Therefore, while organizations may attempt to adopt JIT practice, they need these factors in place for it to be successful, which may justify the criticality indicated in this study.
Lean six-sigma practice is identified as critical in at least two scenarios for both healthcare providers and the pharmaceutical distributor but does not appear for the pharmaceutical producer. It is noteworthy that the producer consistently invests in six sigma training and projects for its employees, indicating a high level of integration and maturity in utilizing six-sigma methodologies within its operations. This situation contrasts with the healthcare providers and the pharmaceutical distributor, highlighting a discrepancy in the adoption and implementation of six sigma across different segments of the supply chain. While the producer has effectively embedded lean six sigma principles to optimize quality and efficiency, healthcare providers and the distributor may not have reached the same level of implementation. Marolla et al. (2022) support these findings by attributing low adoption of lean six-sigma practices in three Italian public hospitals to barriers such as flawed integration of lean and six-sigma methodologies, exacerbated by complex healthcare structures (Thomas and Suresh, 2024). Additionally, Marolla et al. (2022) pinpoint critical factors such as the commitment of top and middle management, robust leadership and emphasize the importance of knowledge of statistical language and tools by the organizations. Building on these insights, Kuiper et al. (2022) affirm that the application of lean six-sigma may inadvertently reduce an organization’s responsiveness to disruptions like a pandemic. Also, Kuiper et al. (2022) emphasize the value of agile methodologies in providing quick responses and suggest that healthcare organizations should focus more on speed and flexibility to increase the resilience of operations, rather than solely on waste reduction and cost efficiency. In summary, for lean six-sigma to be effective, healthcare organizations must invest in leadership, training and proper integration of these practices, which may justify the criticality indicated in this study.
Undoubtedly, the resilience capability of anticipation emerges as the most critical across all levels of the healthcare supply chain and practically all scenarios. This capability, which involves forecasting potential disruptions and preparing strategies in advance to mitigate their impacts, is identified as significantly lacking across healthcare providers, pharmaceutical distributors and pharmaceutical producers. Enhancing this capability is not merely about risk management, rather creating a proactive and agile healthcare supply chain capable of adapting to changes and challenges swiftly and effectively (Pettit et al., 2013). The findings are supported by previous research as the study of Tortorella et al. (2023), which shows through their survey with 106 healthcare supply chain workers that resilience capabilities related to anticipation and monitoring (i.e. proactive capabilities) are less adopted than, for example, adaptability (reactive capability). Additionally, Alemsan et al. (2022) corroborate these findings, highlighting in their scoping review that anticipation is the resilience capability with the fewest studies within the healthcare supply chain context, further emphasizing the need for more focused research and implementation efforts in this area.
VSM is a practice widely adopted across all types of organizations and scenarios (Tlapa et al., 2022), except for pharmaceutical distributors during high-probability events. The lack of criticality of this lean practice aligns with studies showing that VSM is the most used technique for reducing costs and eliminating waste in the healthcare supply chain, according to the literature reviews by Khorasani et al. (2020) and Akmal et al. (2020). In contrast to this work, Abideen and Mohamad (2020) demonstrate the successful application of VSM in a pharmaceutical distribution center and this indicates that healthcare organizations do not have a problem adopting VSM, and the lack of adoption by distributors could potentially be easily resolved with targeted interventions.
6. Conclusions
The objective of this work was to analyze the deployment of lean practices and resilience capabilities within the healthcare supply chain across different disruptive scenarios. The study was conducted as a case study within four Italian organizations: two healthcare providers, a pharmaceutical distributor and a pharmaceutical producer, collectively representing the healthcare supply chain. Based on the work by Alemsan et al. (2022), a questionnaire was developed to evaluate the adoption level of lean practices and resilience capabilities, garnering a total of 100 responses. Also, experts evaluated the importance level of each lean practice and resilience capability in four disruptive scenarios. From these data, it was possible to identify the most critical lean practices and resilience capabilities for each disruptive scenario. Our findings have implications for both theory and practice, being discussed below.
6.1 Theoretical implications
Regarding theoretical implications, this research systematically identified critical lean practices and resilience capabilities that are underutilized at various tier levels within the healthcare supply chain. The study highlighted significant opportunities for theoretical advancement in operational efficiency and system robustness during disruptions. Additionally, the study introduced a novel methodological approach to evaluate the effectiveness of lean and resilience practices across different disruptive scenarios, thereby enriching the theoretical framework for crisis management within healthcare operations. By identifying critical lean practices and resilience capabilities, this research guides further studies to explore these areas and understand their interrelationships across all levels of the healthcare supply chain. We underscored the importance and potential of cross-tier collaboration within healthcare supply chains, providing a theoretical basis for understanding how different tiers can interact more effectively to enhance overall performance.
6.2 Practical contributions
The research provided practical contributions by highlighting some crucial roles, for example JIT practice and anticipation capability, in bolstering the performance of the entire healthcare supply chain. The study also introduced a scenario analysis framework, enabling organizations to assess and strategize against potential disruptions systematically. These insights not only aid in enhancing operational efficiency and resilience but also support the continuous delivery of high-quality patient care. The study also provided information to formulate strategies to guide managers and prioritize practices and capabilities in order to navigate disruptions towards more efficient supply chain operations. This enables a systemic view of the healthcare supply chain, encouraging an understanding of how each organization contributes to the whole supply chain, rather than solely focusing on individual organizational performance.
6.3 Limitations and future research
It is important to acknowledge some limitations of this study. The case study was conducted within the context of the Italian healthcare supply chain, limiting the generalizability of the findings to other countries and healthcare systems. Future studies could address these geographical disparities to enhance the robustness of the theoretical and practical applications suggested. The focus on a single value stream and the sample size also present limitations. To mitigate these limitations, future research should consider expanding the scope of investigation to include multiple value streams and assess more healthcare organizations. Additionally, the analysis of disruptive scenarios, while comprehensive, was constrained by the subjective assessment of probability and consequence, which could vary significantly in real-world situations. Future studies could adopt quantitative assessment models that use statistical or mathematical formulations to estimate the likelihood and potential impacts of disruptions, such as Monte Carlo simulations, fault tree analysis or Bayesian networks.
References
Further reading
Appendix Questionnaire