

Epidemics and pandemics can result in sudden morbidity and mortality as well as social and economic disruption. However, the humanitarian logistics and supply chain management (HLSCM) field has been mostly focusing on life saving operations after natural disasters such as earthquakes and hurricanes. There is no research within the HLSCM literature neither on the unique properties of vulnerable groups, nor their underlying risk factors or how to mitigate them. The COVID-19 pandemic highlighted the uniqueness of some vulnerable groups and motivated us to conduct a structured literature review to identify research needs in HLSCM with regards to vulnerable populations.
The authors conduct a systematic review of literature on the intersection of epidemics/pandemics, humanitarian operations and vulnerable populations. They utilize the Scopus database to search for peer-reviewed journal articles published in English. Our search results in 366 articles which we reduced to 139 after filtering.
There is no research within the HLSCM literature on the unique properties of various vulnerable populations. The authors show that HLSCM scholars can contribute to literature by investigating operational and logistical challenges of serving vulnerable populations through multi-disciplinary research, research on the intersection of public health and supply chain management, research on the intersection of ethics and operations management, and research on cross-sectoral partnerships.
The authors’ work is limited to peer-reviewed journal articles published in English. They did not include books, conference proceedings and think-tank or NGO reports. However, the authors do recognize that these sources can be very valuable.
To best of authors’ knowledge, this is the first study to review the literature on vulnerable populations under the threat of epidemics and pandemics.
1. Introduction
Large scale emergencies and catastrophic events overwhelm the local response capacity and threaten human life. They become disasters when they impact people, cause disruptions of social order and cultural protections, and disproportionably harm vulnerable populations (Quarantelli, 1999). The humanitarian logistics and supply chain management (HLSCM) field has been mostly focusing on life saving operations after natural disasters such as earthquakes and hurricanes (Kunz and Reiner, 2012). It is generally understood that people displaced due to a natural disaster, famine or armed conflict are indeed vulnerable. However, HLSCM research tends to treat them all as one homogenous group and only limited studies exist about the vulnerabilities of people. Research on serving specific vulnerable populations and their needs is scant within the HLSCM literature.
The International Federation of Red Cross and Red Crescent Societies (IFRC) lists epidemics and pandemics among such catastrophic events (www.ifrc.org). Epidemics and pandemics can result in sudden morbidity and mortality as well as social and economic disruption. A recent report published by the United Nations Conference on Trade and Development (UNCTAD) estimates that the COVID-19 pandemic may push an additional 130 Million people to extreme poverty and contract the global economy by 4.3% in 2020 (UNCTAD, 2020). As of 5 December 2020, John Hopkins University Coronavirus Resource Center reports 66.3 Million confirmed global COVID-19 cases and 1.5 million deaths (http://coronavirus.jhu.edu). The COVID-19 crisis has showed that there is a need to expand the discussion on humanitarian operations and logistics into public health crises, especially epidemics and pandemics. The impact of an epidemic or pandemic is exacerbated for vulnerable populations as they may be at higher risk for acquiring the disease and do not always have access to proper healthcare and social services. Moreover, while all epidemics and pandemics present different challenges, the severity and novelty of the COVID-19 pandemic, the pathogenesis of which is still not fully understood to date, brought extraordinary measures like social distancing, lockdowns, stay-at-home orders, school closures and business closures.
Unfortunately, these public health measures have resulted in additional unique, unintended consequences and vulnerabilities such as mental health problems, exploitation and domestic abuse. As businesses remain closed and consumers are stuck at home, mental health problems arise (Pfefferbaum and North, 2020). Vulnerable populations like the world's extremely poor, refugees and migrant workers are prone to exploitation by property owners, employers, gangs and even in some cases government officials (Crippa, 2020). Women and children stuck at toxic home environments are being abused by their own family members (Bradbury-Jones and Isham, 2020; Bettinger-Lopez and Bro, 2020). Considering the complex nature of the COVID-19 pandemic, it is rather crucial that we learn from other disciplines to serve vulnerable populations appropriately. Any humanitarian response to a pandemic such as COVID-19 - or to any natural or man-made catastrophe for that matter – should incorporate logistical contingencies specific to different vulnerable groups.
Our primary objective with this paper is to create awareness among HLSCM researchers about the peculiarities of different vulnerable groups. Their specific needs may affect the planning and execution of humanitarian operations and logistics. We hope to start a conversation within this community about vulnerable groups and their individual needs. Utilizing the disaster management cycle as an analytical framework this paper provides a structured review of literature from relevant disciplines to guide humanitarian logistics researchers in finding potentially impactful research directions related to helping vulnerable populations. Hence our research question is, “what are impactful research directions HLSCM researchers can tackle concerning vulnerable populations”? We investigate work from various disciplines ranging from epidemiology to social sciences and categorize them in the areas of health, social welfare and crime/security for each stage of the disaster management cycle (i.e. mitigation, preparedness, response and recovery). We research pathways in this typology that increase the risk and magnitude of these vulnerabilities, identify research gaps and provide future research directions for integrated cycle of epidemic/pandemic prevention, response and recovery.
The humanitarian community is guided by three principles: humanity (alleviate human suffering), neutrality (help without bias) and impartiality (do not discriminate) (Van Wassenhove, 2006). These principles help setup the main frame of any humanitarian intervention. However, when it comes to execution the devil is in the details. Human life is too precious to rely on blanket programs and generalizations. Not understanding the special needs of different vulnerable groups may lead to disaster within a disaster. For example, lockdowns to control the spread of the virus have inflamed already existing mental health problems and intimate partner violence. Separately, we knew that the elderly were particularly vulnerable to the coronavirus but still failed in our response leading to devastation in hospices and retirement homes. These examples show that the humanitarian community needs to pay more attention to vulnerable populations. We hope this paper becomes the spark that ignites a novel stream of research within the HLSCM community, and thus indirectly helps practitioners and policy makers make informed decisions when helping vulnerable groups in future epidemics and pandemics.
The rest of the paper is organized into following sections. Section 2 explains the steps of the research methodology utilized for this systematic literature review. Section 3 presents the results. Section 4 identifies research gaps and future research directions for humanitarian logistics and supply chain management scholars. Section 5 explains the limitations of the study and concludes the paper.
2. A structured review of literature
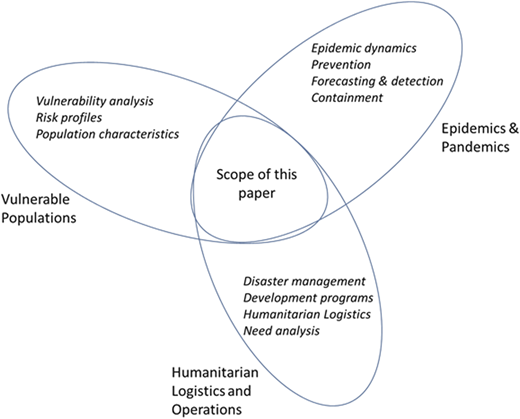
In this study, our aim is to guide humanitarian logistics researchers in finding potentially impactful research directions related to helping vulnerable populations. Utilizing the disaster management cycle as an analytical framework we take on a structured review of literature of relevant disciplines to identify research gaps on vulnerable populations in response to large public health crises such as the COVID-19 pandemic. Figure 1 illustrates the scope of our research. We start this section with defining the three axes, the intersection of which makes up the scope of our literature review. We then explain our search strategy, exclusion criteria and analysis of findings.
2.1 Definitions
Before presenting the details of the research methodology, we outline the different terminologies used in this study for public health crisis and vulnerability.
2.1.1 Humanitarian logistics and operations
The first axis of our literature review is humanitarian logistics and operations. This axis consists of a collection of activities including humanitarian logistics (generally considered as life-saving and emergency relief operations), operations for development programs, and disaster management. Altay and Green (2006) define disaster management as “the set of activities that are performed before, during, and after a disaster to prevent loss of life, reduce the impact on the economy, and returning to a state of normalcy as disaster operations” (p. 476). Before a disaster, communities work on mitigation and preparedness activities. During and immediately after a disaster response operations are executed. Finally, after the disaster response phase is over, recovery and reconstruction efforts start. For more detailed information on the specific activities within each stage disaster management the reader is referred to Altay and Green (2006).
Humanitarian logistics and operations is an area that borrows from the fields of logistics, supply chain management and operations management (Van Wassenhove, 2006). Thomas and Kopczak (2005) define humanitarian logistics as “the process of planning, implementing and controlling the efficient, cost-effective flow and storage of goods and materials, as well as related information, from the point of origin to the point of consumption for the purpose of alleviating the suffering of vulnerable people” (p. 2). The field is generally concerned about coordination, allocation, movement and procurement of resources (i.e. physical goods, human resources as well as information) in order to help people in need.
2.1.2 Public health crisis
We should note that while the terminology used in managing and controlling a public health crisis is similar to the disaster management cycle, there are differences in the meaning of terms. We first define the terms related to public health crisis below using definitions from the Center for Disease Control (CDC):
Endemic is the baseline level of a disease present in a community.
Outbreak refers to a greater-than-anticipated increase in the number of endemic cases, often for a limited geographic region.
Epidemic refers to an increase in the number of cases similar to an outbreak but for a larger geographic area.
Pandemic is an epidemic that has spread over several countries or continents.
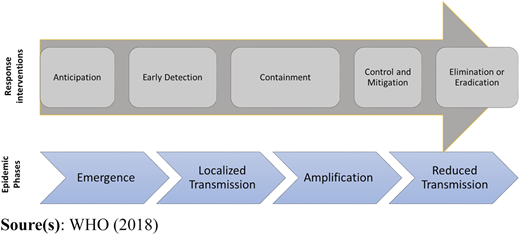
Based on these definitions we can see that the type of health crisis depends on the dynamics of the disease, occurrence level and geographic spread. Figure 2 shows the phases of epidemics dynamics and outlines the types of response and interventions: anticipation, early detection, containment of the disease, control/mitigation and elimination/eradication. The phases of infectious disease threats start with introduction or emergence of the virus in a community. Anticipation includes forecasting of the most likely diseases to emerge or re-emerge, and preparedness for a variety of scenarios. Early detection of a disease requires laboratory confirmation of new and re-emerging cases in animal and human populations to enable implementation of rapid containment measures. In the second phase, an outbreak with localized transmission starts, which then amplifies into an epidemic or pandemic in the third (amplification) phase. Once the disease is amplified to an epidemic or pandemic level, interventions focus on control and mitigation strategies to reduce the impact on health, economic, political, and social systems. In the last phase, assuming interventions are successful, transmission is reduced, risk of outbreak is eliminated, and the infectious disease is eradicated. In this research, we focus on diseases, which go to the third phase and beyond. Examples of public health crises caused by novel viruses include HIV, Influenza A virus subtype H1N1 and H5N1, SARS-CoV1, MERS-CoV, Ebola and the ongoing COVID-19.
2.1.3 Vulnerability
In order to protect, plan and serve vulnerable populations better during epidemics and pandemics, we need to define vulnerability, understand its determinants and the unique needs of vulnerable populations. In social science and public health literature, vulnerable, at-risk and special are different terms used to describe vulnerable people (Cutter et al., 2003; Hutchins et al., 2009; Shi and Stevens, 2010). Cutter et al. (2003) describe vulnerability as potential for loss, while Wolf et al. (2013) define it as a measure of potential prospective harm. In public health, Shi and Stevens (2010) describe vulnerable populations as people at higher risk for poor health and with limited access to health care. In disaster management, risk is described as the potential loss due to a hazard and is a function of vulnerability and exposure to the hazard (Cardona et al., 2012). Loss can be related to human lives, property or financial costs (Burton, 1978; Cardona, 2005).
The United States National Response Framework uses a functional approach to define different services needed by at-risk persons before, during, and after an incident. These functional areas include maintaining health, independence, communication, transportation, support services, medical care and self-determination (FEMA, 2019). Among individuals who might need additional support are children, elderly, individuals with disabilities, those who live in institutionalized settings, people from diverse backgrounds and have limited local native language proficiency, or are transportation disadvantaged. Hutchins et al. (2009) discuss a population-based approach to identify vulnerable groups by a variety of geographic, demographic, biological, cultural, or socioeconomic characteristics such as age, race/ethnicity, income and housing. They identify the following as vulnerable populations for an influenza pandemic in the US: pregnant women, children, people with disabilities, public-housing residents, single-parent families, low-income populations, immigrants and refugees, jail facilities and their residents, farm workers, racial/ethnic minorities, home healthcare workers, and tribal communities (Hutchins et al., 2009). This literature review identifies additional at-risk persons, such as people with underlying health conditions (especially people with autoimmune diseases and comorbidity), first responders and other healthcare personnel, which will be discussed further in Section 3.
2.2 Search strategy
For this systematic literature review, we follow the steps outlined in Altay and Green (2006), Gupta et al. (2019) and Banomyong et al. (2019). We utilize the Scopus database for this review because it is the largest abstract and citation database of peer-reviewed literature with over 77.8 Million records (www.scopus.com). This research focuses on the intersection of public health crises, vulnerable populations and humanitarian operations to serve these populations. Using the definitions in Section 2.1, we identify different search terms that may be used in four thematic areas, namely “health crisis,” “vulnerability,” “service” and “humanitarian.” Table 1 lists the search terms used in identifying potential articles for the review. The search terms in Table 1 are combined using Boolean operators (AND, OR) and searched in article title, abstract and author-generated keywords. We first use the operator OR to combine the keywords in the same thematic area (e.g. epidemic OR pandemic, etc.), and then utilize the AND operator to combine the search terms in four thematic areas. Table 2 shows the syntax used in the search.
Search terms used in the study
| Health crisis | Vulnerability | Service | HLSCM |
|---|---|---|---|
| Epidemic | Vulnerable | Serve | Logistics |
| Pandemic | At-risk | Need | Supply chain |
| Outbreak | Special need | Prepare | Operations |
| Health disaster | Special population | Response | |
| Health crisis | Recover | ||
| Mitigate | |||
| Containment | |||
| Elimination | |||
| Eradication |
Search syntax
| Data source | Search syntax |
|---|---|
| Scopus Database: July, 2020 | ((TITLE-ABS-KEY (“epidemic”) OR TITLE-ABS-KEY (“pandemic”) OR TITLE-ABS-KEY (“health disaster”) OR TITLE-ABS-KEY (“health crisis”) OR TITLE-ABS-KEY (“outbreak”)) AND (TITLE-ABS-KEY (vulnerable) OR TITLE-ABS-KEY (“special need”) OR TITLE-ABS-KEY (“special population”) OR TITLE-ABS-KEY (“at risk”)) AND (TITLE-ABS-KEY (response) OR TITLE-ABS-KEY (prepare) OR TITLE-ABS-KEY (mitigate) OR TITLE-ABS-KEY (eliminate) OR TITLE-ABS-KEY (eradicate) OR TITLE-ABS-KEY (contain) OR TITLE-ABS-KEY (control) OR TITLE-ABS-KEY (detect)) AND (TITLE-ABS-KEY (operations) OR TITLE-ABS-KEY (“supply chain”) OR TITLE-ABS-KEY (“humanitarian”) OR TITLE-ABS-KEY (“logistics”))) AND (LIMIT-TO (DOCTYPE , “ar”) OR LIMIT-TO (DOCTYPE , “re”)) AND (LIMIT-TO (LANGUAGE , “English”)) |
Similar to Nurmala et al. (2017), we limit our attention to published or in-press, peer-reviewed journal articles written in English language. Furthermore, as suggested by Altay and Green (2006) and Gupta et al. (2019), conference proceedings, book chapters and books do not always go through the peer-review process, and therefore were not considered. The search was performed in July 2020 and covered the entire timeframe available in Scopus until that point (the oldest record in Scopus dates back to 1788).
2.3 Exclusion criteria
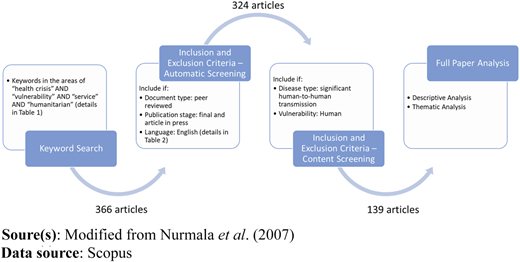
The syntax presented in Table 2 results in 366 papers. We next develop and apply inclusion and exclusion criteria with respect to content to select papers for analysis. We only include papers related to infectious diseases that have significant human-to-human transmission component using CDC's list of infectious diseases (https://www.cdc.gov/nchs/fastats/infectious-immune.htm). As a result, we exclude papers related to chronic diseases and conditions such as obesity, diabetes; food-borne and vector-borne diseases that only have animal-to-human transmission or rare-human-to human transmission such as salmonella, dengue fever, and malaria. Additionally, the focus of the review is human vulnerability thus we exclude papers related to supply chain or computer system vulnerability. As a result of this content screening, we identify 324 studies that fit the overall review criteria. Next, these papers are independently screened by the authors of this study, reading the abstracts and when necessary the papers themselves carefully, to decide on their appropriateness for this study. During this read-through step disease types, vulnerable populations, risk factors and stages of the disaster cycle/disease dynamics are coded. Exclusion and coding decisions are then discussed among the authors until a consensus has been reached. This process eliminated 185 more studies, resulting in the final pool of 139 papers. A significant number of eliminations include papers that mention “vulnerable population” or “at-risk people” in the abstract but then do not specify a group of people or has nothing to do with service, operations, logistics or supply chain. Figure 3 presents the steps of the paper selection process.
An interesting observation about the final 139 papers is that none of them is published within the HLSCM field, thus providing justification for this paper. The fact that humanitarian logistics and supply chain researchers have not paid attention to the special needs of different vulnerable populations may suggest that the models developed to help people in need are generalized action plans missing the individuals on the periphery.
2.4 Analysis
We analyze the papers by year, discipline, vulnerable population, risk type, disaster management stage and epidemic dynamics phase. We categorize sources of risk for vulnerable populations mentioned in the papers into three groups: health, economic and security. Examples for each category include worsening of medical condition, costs incurred, and exploitation, respectively. These categories can be interrelated. We also group papers based on their focus on the disaster management framework as well as epidemic dynamics.
3. Findings of the review
This literature review makes two main high-level contributions to the HLSCM literature. First, it identifies research gaps that pertain to serving vulnerable populations during epidemics/pandemics. Second, it offers HLSCM scholars four research streams to expand research on vulnerable populations. In this section, we focus on our first contribution. Section 4 will present the four research streams we propose.
The most obvious result of our analysis of the 139 final papers is that there are no papers within the HLSCM and production/operations management literatures on specific needs of, as well as the tactics and strategies to help, various vulnerable populations. Majority of the papers in the final set come from medical, public health and social sciences literatures. The full list of the journals in the final set can be found in the Appendix.
When we search for “vulnerable populations” in the HLSCM literature, we see that they are very generally described as people affected by a disastrous event, or “at-risk” people in an epidemic or pandemic without going into any specifics about their unique characteristics. This aggregate approach is understandable as it allows scholars to develop operations models or strategies that would generally work for all affected people. Unfortunately, vulnerable groups tend to have specific needs and constraints that set them apart. For example, helping senior citizens in a nursing home presents different challenges than helping infants in a maternity ward. Consequently, we first identify the vulnerable groups covered in the final pool of papers and organize them into eight categories based on their commonalities in our subjective opinion: Age, occupation, living conditions, people on the move, social status, mental health, physical health, and gender/sexual orientation. We should note that these vulnerable population categories presented in Table 3 are organized heuristically with an operations/logistics lens in mind. For example, it could be argued that being disabled is a physical challenge, and should be listed in the “physical health” category. We do not disagree. Unfortunately, disability also has a social stigma attached to it in some societies, especially those that are not disabled-friendly, and assistance should be respectful and dignified. A similar argument can be made for homelessness, which can be considered a social status or a living condition. In this paper, we refer to the physical environment when considering living conditions.
Vulnerable groups identified and their frequency count in the final pool of papers
| Age (25) | Adolescents | 6 | Social status (32) | Poor | 9 |
| Young adults | 6 | Racial/ethnic minority | 9 | ||
| Elderly | 6 | Social disparity | 5 | ||
| Children | 5 | Homeless | 5 | ||
| Infants | 2 | Slave labor | 1 | ||
| Occupation (24) | Healthcare workers | 12 | Food insecure | 1 | |
| Sex workers | 6 | Disabled | 1 | ||
| Military personnel | 2 | Orphans | 1 | ||
| Female humanitarian workers | 1 | Mental health (23) | Injection drug users (IDU) | 14 | |
| Micro-farmers | 1 | Drug users | 5 | ||
| Nannies | 1 | Mental health | 3 | ||
| Unemployed | 1 | Developmental disabilities | 1 | ||
| Living conditions (11) | Rural settlements | 4 | Physical health (20) | Pre-existing conditions | 6 |
| Immunocompromised | 4 | ||||
| Nursing home residents | 3 | Unvaccinated | 3 | ||
| Informal settlement residents | 1 | Comorbidity | 2 | ||
| Remote/offshore operations | 1 | Pregnant women | 2 | ||
| University residences | 1 | Dialysis patients | 1 | ||
| Homebound patients | 1 | TB patients | 1 | ||
| People on the move (21) | Refugees/IDPs* | 12 | Critically ill | 1 | |
| Gender/Sexual orientation (25) | Homosexual men | 13 | |||
| Migrants | 6 | Women | 11 | ||
| Travelers | 3 | LGBTQ | 1 |
Note(s): *IDP = internally displaced people
Categories in Table 3 roughly have equal coverage (the numbers in parentheses are the frequency counts for each category). Social status has been covered more than others, with racial/ethnic minorities, people living in poverty or experiencing social disparity (e.g. cast system in India), and homeless people, drawing the most research in this category. Living conditions is the least covered topic, which is surprising because one's physical surroundings is generally expected to be a source of vulnerability (e.g. having a home vs living in a tent or a homeless shelter). These categories are not mutually exclusive and intersections of them can create very specific vulnerable populations. For example, pregnant adolescent women living in a refugee camp would be covered by age, living conditions, and gender/sexual orientation categories. A careful reader will quickly realize that the sum of the counts in Table 3 exceeds the number of papers in the final pool. This is due to two reasons: first, some studies consider multiple vulnerable groups, and second, some vulnerable populations mentioned in the reviewed papers can be categorized in multiple groups without losing the characteristics of either group (similar to disjoint sets). A good example is migrant sex workers. We count this group twice, once for “migrants” and again for “sex workers” because each group has distinctly different and unique operational needs.
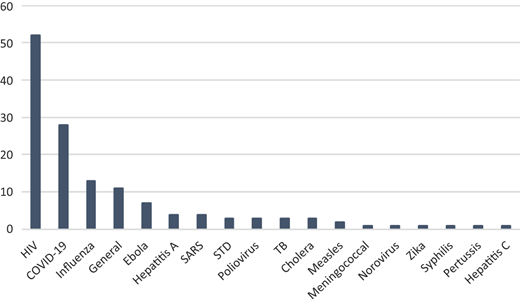
The disease with the most coverage in the final pool of articles is HIV with 51 papers. Four diseases, namely HIV, COVID-19, Influenza and General make up 75% of all the papers reviewed. When a paper does not specify a particular disease but considers a generic epidemic or pandemic's impact on a particular at-risk population, we categorize the disease as “general.” Even if we remove COVID-19 papers from the final pool of papers (since this pandemic overwhelmed publications in 2020), HIV, Influenza and General still cover 68% of the papers. Figure 4 shows the frequency of diseases in the papers reviewed.
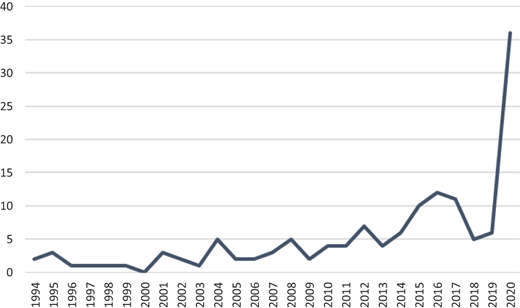
Research on the needs of specific vulnerable populations in the context of infectious diseases has been slowly gaining attention since 1994 with small spikes in 2004 (SARS), 2012 (Influenza), 2016 (Ebola and Polio) and of course 2020 (COVID-19). HIV on the other hand, has been a constant topic of discussion throughout the years. Figure 5 below shows the frequency of papers by publication year. The abnormal jump in 2020 is due to the popularity of COVID-19 as a research topic and arguably due to the fact that it affected the whole world at different intensities and ways.
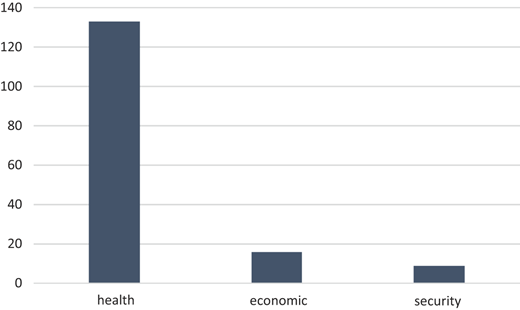
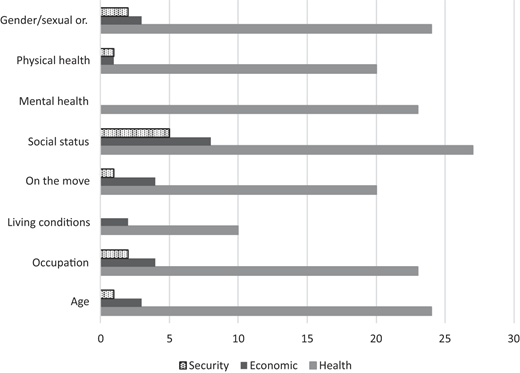
As mentioned in Section 2.4, we categorize sources of risk for vulnerable populations in our literature review into three groups: health, economic and security. Since our review is focused on infectious diseases it is no surprise that vast majority of the papers in the review sample are related to the health risk. Figure 6 shows the frequency of risks appearing in our final review sample. Some papers cover more than one risk factor, thus bringing the total risk count higher than 139, the number of papers in the review sample. When we look into the papers carefully we see that the economic risks are associated with people on the move (refugees/IDPs and migrants), minorities, women, elderly and expectedly, people living in poverty. Security risk on the other hand, is mostly associated with women (sex workers, female humanitarian workers) and children as well as the poor, refugees/IDPs, and those working in bonded labor (i.e. modern slavery).
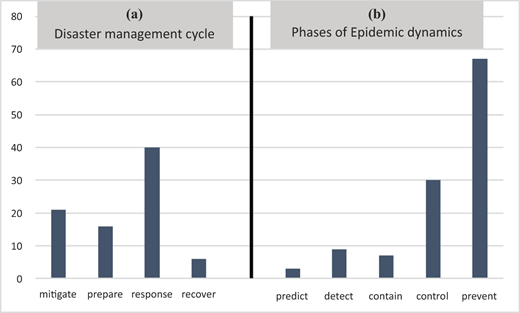
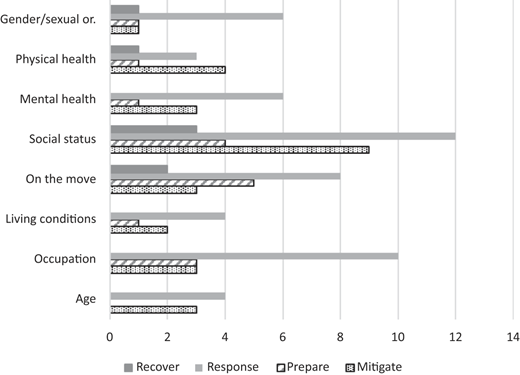
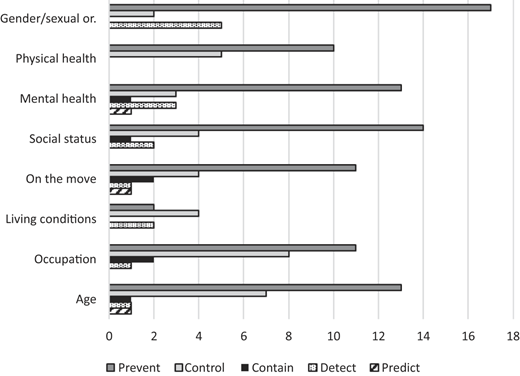
The next part of our analysis is related to the stages of the disaster cycle and epidemic dynamics that have received attention from scholars researching serving vulnerable populations. Figure 7 shows the results of our analysis. Figure 7a shows the frequency count of research on the stages of the disaster management cycle, while Figure 7b focuses on the phases of epidemic dynamics. Research on vulnerable people follows the same trend that disaster management research did for many years, with most of the attention being on the response stage and least on recovery (Altay and Green, 2006). Mitigation and preparedness stages collectively attracted about the same amount of research as the response stage. In terms of epidemic dynamics, most of the research on vulnerable populations is on prevention, most likely because in this phase the risk factors and drivers of risk for specific at-risk groups need to be identified in order to develop effective prevention strategies. We see five times more research on the control and prevention phases than predict, detect and contain phases, collectively.
In the last part of our analysis of the 139 papers, we identify research gaps by cross-referencing the eight vulnerable groups listed in Table 3 to the risk factors (Figure 8), disaster management stages (Figure 9), and phases of epidemic dynamics (Figure 10).
Frequency of papers on the stages of epidemic dynamics within each vulnerable group
Frequency of papers on the stages of epidemic dynamics within each vulnerable group
Figure 8 shows that research on risk factors extensively cover health risk. This of course is expected since this literature review is about helping vulnerable groups under the risk of infectious diseases. The more interesting story in this figure however, is that we did not find any papers that consider security or economic risks for vulnerable groups suffering from mental health issues. Similarly, we did not find any research on security risk within the vulnerable groups defined based on their living conditions/environment. This topic could be of particular interest for HLSCM researchers working on issues related to refugees and IDPs. People running from armed conflict may not have access to formal refugee camps and frequently form informal settlements. For example, refugees of Syrian war have established informal settlements on their way to Europe through Turkey and Greece (Ekathimerini, 2018).
Figure 9 shows research on the four stages of the disaster management cycle as they relate to vulnerable groups. The dominant stage researched in our final pool of papers immediately evident in Figure 9 is the response stage. What is missing is research on recovery, especially concerning vulnerable groups identified with mental health, living conditions, occupation and age. The less obvious observation from Figure 9 is that preparedness is underrepresented and ranks third among the four stages. We find this lack of interest in preparedness surprising because it is generally accepted within the HLSCM community that money spent on preparedness reduces spending in response (Wade, 2011; Jamieson, 2016). Therefore, more research on preparedness may have a big impact on helping vulnerable populations during a response operation. For example, COVID-19 wreaked havoc among the elderly living in nursing homes and assisted living facilities (https://www.cdc.gov/mmwr/volumes/69/wr/mm6946a3.htm). Preparing these facilities for social distancing, stocking up masks, hand sanitizers and disinfectants, upgrading HVAC filtering systems and increasing the frequency of decontamination of common spaces could have made a difference in the death toll. Of course, we are only speculating here, and this is why more research is needed on preparedness in the context of helping different vulnerable populations.
Lastly, Figure 10 presents the results of cross-referencing vulnerable groups from Table 3 with the five stages of epidemic dynamics. What is immediately obvious is that prevention research is aplenty. However, two stages are in need of further research, namely, containment and prediction. We see great potential here for HLSCM scholars, as the former requires logistics expertise and the latter forecasting. Among the vulnerable groups, the one that attracted the least research are groups identified by their living conditions. Groups identified by their physical health only attracted research on control and prevention and need more research on prediction, detection and containment.
A close look at the final pool of papers reveals that the majority of the research is about understanding the risk factors for vulnerable populations. This is indeed an essential step for preventing disease spread among at-risk people, but if the prevention is not successful and the disease is amplified, then response strategies need to be customized for different vulnerable groups. For example, research on refugees/IDPs is primarily on prevention and response. Research on control of spread among various vulnerable groups primarily comes from the medical literature, while research on responding to different needs of vulnerable groups generally comes from social sciences. There is very little research outside of the medical and public health fields in the final pool of papers. The handful of papers (only nine) outside of these two scholarly fields tend to focus on the preparedness and response strategies to health and economic risks for refugee/IDPs and people living in extreme poverty. These papers deal with HIV, Ebola and COVID-19 with half of them in the context of complex emergencies. Another interesting finding is that majority of these papers have been published in 2019–2020 showing that scholars outside of the medical and public health fields have started showing interest in research on vulnerable populations. In the next section, we provide research directions to catalyze research on vulnerable populations within the HLSCM community.
4. Research gaps and needs
Our literature review shows that within the humanitarian operations, logistics and supply chain literatures there is virtually no research on the vulnerabilities of at-risk populations and their operational and logistical implications. It is difficult to propose future research directions when there is virtually no research done on this specific area. Therefore, we develop four research areas based on our experience in the field, our interactions with practitioners and current trends in humanitarian logistics research: (1) multi-disciplinary research; (2) intersection of public health and supply chain management; (3) intersection of ethics and operations management in the context of serving vulnerable populations; and (4) cross-sectoral partnerships on helping vulnerable populations during an epidemic or pandemic.
Our literature review identified eight vulnerable populations (Table 3) and confirmed that they are highly susceptible to epidemics and pandemics due to the three risk factors shown in Figure 6. Their circumstances tend to create unique needs, and therefore call for targeted interventions rather than blanket public health policies. To clarify, we are not suggesting that blanket public health policies are ineffective. They certainly work for the majority of the population. Nevertheless, relatively smaller groups of individuals do have unique needs that are specific to their situation, thus resulting is a wide array of needs to be considered.
No single government agency or humanitarian organization is completely equipped (structurally, emotionally, or resource-wise) to respond to each of these groups. This means assisting vulnerable populations requires an inter-disciplinary approach (research area 1) (Halbreich et al., 2019). Better yet, policies developed for vulnerable groups should be supported by law (Runge, 2013) and integrated into the regional and national public health response strategies (Renne, 2018). Hence, national or regional resources can be channeled to local interventions since local NGOs and government institutions are closer to the populations in need of assistance. Execution and delivery of these public health programs (research area 2) will require partnerships between these organizations (research area 4). Finally, the public health programs geared towards specific vulnerable groups have to be fair and equitable, which is likely to push policy makers to think about solutions and processes on the intersection of ethics and operations management (research area 3).
In the paragraphs below, based on the four research directions we identified, we attempt to provide some specific research ideas for HLSCM scholars to start the conversation on vulnerabilities and populations at-risk.
4.1 Multi-disciplinary research
Humanitarian operations in general is an interdisciplinary subject because from the declaration of an emergency to funding to resource allocation various organizations and individuals from different disciplines get involved in the planning and execution of humanitarian assistance and development programs. Vulnerabilities further expand this need for multidisciplinary research because depending on the underlying risk factors of a vulnerability, social scientists, ethicists, scholars of medicine and public health, epidemiologists and others will have valid and critical inputs. Bedford et al. (2019) also invite multi-disciplinary research on vulnerable populations, “including not only epidemiology but also social sciences, research and development, diplomacy, logistics and crisis management” (p. 130). One such example is the development of vulnerability indexes and maps. Geospatial information is critical in the delivery of assistance to vulnerable populations but this data generally ignores specific information relevant to the vulnerable population hindering targeted intervention. Stanturf et al. (2015) develop a vulnerability index using census data and use it in Liberia to identify vulnerability hotspots. Such indexes and vulnerability maps create situational awareness, allowing policy makers and responders to allocate resources properly, and develop effective prevention and containment strategies. They provide an opportunity to incorporate operations and supply chain specific requirements into an index along with vulnerability-specific data, thus producing a more complete, well-rounded picture of the situation.
4.2 Intersection of public health and supply chain management
The COVID-19 pandemic showed us that public health systems cannot function without resilient, agile, yet efficient supply chains. Shortages of N95 face masks, personal protective equipment (PPE), and ventilators not only made the job of healthcare workers more difficult than it already is, but also increased their risk of exposure, creating a completely new group of vulnerable people (Wingfield and Taegtmeyer, 2020). Separate from healthcare supply chains, the supply chain of providing relief to migrants, refugees and IDPs presents completely different challenges. While migrants and some refugees are on the move, others along with IDPs are stuck in camps. The logistics of serving these two groups (i.e. on-the-move vs in-a-camp) is fundamentally different (Oloruntoba and Banomyong, 2018). COVID-19 created a similar challenge for people who are stuck in one place, such as senior citizens in nursing homes or people on the move, such as air travelers and migrant workers. These supply chain challenges are increasingly being recognized among scholars outside of the supply chain management/logistics fields. For example, Lau et al. (2020) draw attention to supply chain management issues based on their experience with Ebola, SARS and MERS. They point out that “indirect health effects exceeds the death and morbidity caused by the disease” (p. 647) and ensuring the continuity of health services and prevention programs relies of effective and sustainable supply chain operations. Similarly, CDC calls for integrated services that are cost effective and logistically feasible targeting vulnerable populations (Pinto et al., 2018). Thus, it is clear that supply chain and logistics should be part of the discussion when it comes to public health planning and execution (Bedford et al., 2019).
From an operations research/management science (OR/MS) perspective, the models on the intersection of public health and supply chain management will need to have novel constraints, which take into consideration the unique properties of vulnerabilities being studied. Similarly, it is not clear if the traditional cost minimization objective would fit the needs of models for vulnerable populations. Similar to Holguin-Veras et al. (2013) who introduced deprivation cost to the HLSCM literature, we need to investigate and understand the “cost function” for the management of vulnerabilities. For example, one vulnerable group with unique operational challenges are dialysis patients. Effectively helping dialysis patients during and after a disaster or pandemic requires coordination with health professionals and emergency managers as lack of clean water, power outages, and transportation difficulties can disrupt dialysis care (Smith et al., 2020). In addition, social disparities amplified by COVID-19 call for equitable dialysis care (Morton et al., 2016), which is unlikely to be modeled using a cost minimization objective function.
4.3 Intersection of ethics and operations management
The risk factors we categorized in Table 3 not only present operational and logistical challenges but also ethical ones. For example, prioritization of vaccinations should be considered in the context of equity and impartiality. Similarly, the interaction between public health and safety measures such as social distancing, school and business closures, and return-to-work decisions all require careful review as various vulnerable groups could suffer from unintended consequences. Furthermore, communication of risks to different at-risk groups is critical for everyone to understand the purpose and intention of intervention plans. Clear and transparent communication will minimize misinformation and build trust (Lau et al., 2020). This proves an opportunity to extend the research on swift trust (Tatham and Kovacs, 2010; Dubey et al., 2019; Schiffling et al., 2020) into vulnerable communities in the context of a pandemic.
The unique nature of each vulnerability presented in Table 3 requires customized approaches that are sensitive to the needs of the corresponding vulnerable groups. Gender-based approaches provide one such example. One side effect of the stay-at-home orders during COVID-19 is the increase in domestic violence (Bradbury-Jones and Isham, 2020). Unfortunately, violence against women is an age-old and multi-faceted problem with gender disparities, patriarchy and chauvinism lying in its core, the severity of which is further heightened within chaotic environments such as epidemics, pandemics, disasters and armed conflict. For example, after the 2010 Haiti earthquake it was documented that some women at camps were sexually assaulted while trying to use toilets, which led to a discussion on camp layout and latrine locations (Gerntholtz and Rhoad, 2010). Later, Sommer et al. (2015) argue that the challenge of girls and women being vulnerable to violence while accessing water and sanitation facilities has not been adequately addressed. This could be because camp layout design research is not including the safety of women and girls as a constraint in the model. Hence, layouts of refugee and IDP camps need to be reconsidered based on the safety of women.
In the case of COVID-19, women are being assaulted at home. This is uncharted territory for HLSCM researchers as they are used to modeling relief deliveries to camps, or in the case of the Syrian refugee crisis, to refugees on the move. Similar to the differences between warehouse versus home deliveries, resource allocation, prioritization and dispatch decisions to help victims of domestic violence need to be reevaluated. Gender analysis methodologies from social sciences such as the capacities and vulnerabilities approach (CVA) developed to identify and understand gender inequalities and social power differentials in areas in need of humanitarian interventions can be adapted and applied to epidemics and pandemics (Birks et al., 2017). Research methodologies from the field of HLSCM should be used together with social science methodologies such as the CVA to develop novel problem modeling approaches that are sensitive to equality and equity.
4.4 Cross-sectoral partnerships
One of the interesting challenges of a pandemic is the transition from response to recovery, the timing and duration of which depends on if/when a vaccine becomes available. With natural disasters, a response to a hazardous event is then followed by the relief and recovery stages. In other words, disaster management operations are usually linear in nature. However, the progression of an epidemic or pandemic depends on how well the public health crisis is being managed, and can bounce back and forth between the response and recovery phases. Although this is a unique and interesting problem, there is no literature on this transition, especially when vulnerable populations are of concern (Fakhruddin et al., 2020). This challenge is further exacerbated with the need to respond to natural disasters happening during a pandemic. For example, on July 25, 2020 Hurricane Hanna, a category 1 Hurricane devastated the Rio Grande Valley (i.e. US-Mexico border in South Texas) which was already a hotspot for COVID-19 with all hospitals in the region already at capacity (Cappucci et al., 2020). A Hurricane brings with it additional challenges different from the pandemic. Injured people put the already stretched health system to test. People contaminated with flood waters walking into hospitals add another layer to sanitation challenges. Displaced people gathering in churches, schools and relatives' homes increase disease spread. Flooded roads, downed trees and power lines hinder deliveries of goods and medical equipment. Flood waters may contaminate the public water system and spread disease. All these additional challenges arrive when the public health and emergency management systems are fully focused on managing a pandemic.
As mentioned in Section 4.1 above, research on pandemic response needs to be multi-disciplinary because the problem itself is multi-faceted. This also means that one organization alone is not equipped to handle all of the issues that may rise during a response, or even understand all the issues a vulnerable group is facing. The solution to this problem is cross-sectoral partnerships.
Research on partnerships among organizations from different sectors is not new (Stadtler and Van Wassenhove, 2016). The effectiveness of multi-stakeholder partnerships among NGOs, governmental institutions, and corporations has already been shown in the context of environmental (Pagell and Wu, 2009; Albino et al., 2012) and social sustainability (Kalkanci et al., 2019) projects within supply chains. Cross-sectoral partnerships between business and non-business actors have also been successful in Base of the Pyramid (Hahn and Gold, 2014) and poverty alleviation projects (Rodriguez et al., 2016). Non-business actors can offer complementary, intangible resources such as local market knowledge and facilitate trust among parties involved in cross-sectoral collaborations (Benstead et al., 2018). Within the HLSCM literature cross-sectoral partnerships is a fast growing research topic. Nurmala et al. (2017) and Tomasini (2018) provide excellent reviews of partnerships between humanitarian organizations and corporations. However, there is still need for further research as NGO-corporate partnerships are mostly limited to philanthropy, tend to be dyadic, and focus on disaster response (Nurmala et al., 2018). Thus, there is a clear need for research on cross-sectoral partnerships for the other stages of the disaster management cycle (i.e. mitigation, preparedness and recovery) as well as the phases of epidemic dynamics. Furthermore, research on partnerships in the context of vulnerable groups can help us understand how to respond to their needs more effectively. For example, Brewster et al. (2018) investigate how cross-sectoral partnerships influence social determinants of health for older adults living in nursing homes, and report that local governments that maintained informal partnerships with a broad range of organizations in health care and other sectors had significantly lower hospital readmission rates when compared to governments that did not maintain their partnerships.
5. Conclusions and limitations
Within the HLSCM literature, “vulnerable populations” frequently refer to people in need of help due to an emergency, and research generally does not specify the vulnerabilities of these groups. Unfortunately, vulnerabilities of individuals or populations segments, their underlying risk factors and appropriate mitigation strategies have not been studied in this literature. Neither there is research on the unique needs of different vulnerable groups and tactics/strategies for responding to them. The COVID-19 pandemic highlighted the uniqueness of some vulnerable groups and motivated us to conduct a systematic literature review to identify research needs in HLSCM concerning vulnerable populations. Our review identifies 139 papers from social sciences, medical, public health and development literatures. We first provide descriptive statistics on these papers and then identify four major areas for research.
We show that HLSCM scholars can contribute to literature by investigating operational and logistical challenges of serving vulnerable populations through multi-disciplinary research, research on the intersection of public health and supply chain management, research on the intersection of ethics and operations management, and research on cross-sectoral partnerships.
Our review is limited to peer-reviewed journal articles published in English language. We did not include books, conference proceedings and think-tank or NGO reports. However, we do recognize that these sources can be very valuable. One future enhancement of this research may be to repeat the same analysis after the pandemic ends, but this time expand the search into other sources of information.
Full list of journals and article count in the final set
| Source title (in alphabetical order) | Count |
|---|---|
| Addiction | 1 |
| African Journal of Primary Health Care and Family Medicine | 1 |
| African Journal of Reproductive Health | 1 |
| AIDS | 4 |
| AIDS Care – Psychological and Socio-Medical Aspects of AIDS/HIV | 5 |
| AIDS Research and Human Retroviruses | 1 |
| American Journal of Preventive Medicine | 1 |
| Anaesthesia and Intensive Care | 1 |
| Archives of Medical Research | 1 |
| Asia Pacific Journal of Social Work and Development | 1 |
| Australian and New Zealand Journal of Medicine | 1 |
| BMC Infectious Diseases | 3 |
| BMC International Health and Human Rights | 1 |
| BMC Public Health | 7 |
| BMJ Global Health | 1 |
| Brain Stimulation | 1 |
| Bulletin of the World Health Organization | 1 |
| Canadian Journal of Anesthesia | 1 |
| Canadian Journal of Public Health | 1 |
| Chest | 1 |
| Child Abuse and Neglect | 1 |
| Clinical Infectious Diseases | 1 |
| CMAJ | 2 |
| Critical African Studies | 1 |
| Development and Change | 1 |
| Disasters | 1 |
| Environment, Development and Sustainability | 1 |
| Epidemiology and Infection | 1 |
| European Geriatric Medicine | 1 |
| European Journal of Epidemiology | 1 |
| European Journal of Public Health | 2 |
| Eurosurveillance | 2 |
| Expert Review of Vaccines | 1 |
| Field Actions Science Report | 1 |
| Food Security | 1 |
| Harm Reduction Journal | 1 |
| Harvard International Review | 1 |
| Health Policy and Planning | 1 |
| Health Promotion International | 2 |
| Human Vaccines and Immunotherapeutics | 1 |
| Indian Journal of Community Health | 1 |
| Indian Journal of Community Medicine | 1 |
| Indian journal of public health | 1 |
| Infectious Diseases of Poverty | 1 |
| International Emergency Nursing | 1 |
| International Journal for Equity in Health | 3 |
| International Journal of Drug Policy | 1 |
| International Journal of Environmental Research and Public Health | 2 |
| International Journal of Epidemiology | 1 |
| International Journal of Health Planning and Management | 1 |
| International Journal of STD and AIDS | 1 |
| International Journal of Tuberculosis and Lung Disease | 2 |
| Irish Journal of Psychological Medicine | 1 |
| JAMA Network Open | 1 |
| Journal of Business Continuity and Emergency Planning | 1 |
| Journal of Entrepreneurship in Emerging Economies | 1 |
| Journal of Health Management | 1 |
| Journal of Infectious Diseases | 2 |
| Journal of Medical Internet Research | 1 |
| Journal of Medical Sciences | 1 |
| Journal of Medical Virology | 1 |
| Journal of Public Health Management and Practice | 2 |
| Journal of Risk Research | 1 |
| Journal of the American Geriatrics Society | 1 |
| Journal of the American Medical Association | 1 |
| Journal of the International AIDS Society | 2 |
| Journal of Urban Health | 2 |
| Kaohsiung Journal of Medical Sciences | 1 |
| Military Medicine | 1 |
| Nursing and Health Sciences | 1 |
| Parasites and Vectors | 1 |
| Pediatrics | 1 |
| PLoS Neglected Tropical Diseases | 2 |
| PLoS ONE | 10 |
| PLoS Pathogens | 1 |
| Pneumon | 1 |
| Prehospital and Disaster Medicine | 1 |
| Prehospital Emergency Care | 1 |
| Preventing Chronic Disease | 1 |
| Psychological Medicine | 2 |
| Psychology, Health and Medicine | 1 |
| Public Health Reports | 2 |
| Recenti Progressi in Medicina | 1 |
| Revista Brasileira de Epidemiologia | 1 |
| Scandinavian Journal of Public Health | 1 |
| Sexually Transmitted Diseases | 2 |
| Sexually Transmitted Infections | 1 |
| Social Science and Medicine | 4 |
| South African Medical Journal | 1 |
| SPE Reprint Series | 1 |
| The BMJ | 1 |
| The Canadian Nurse | 1 |
| Tuberculosis | 1 |
| Vaccine | 2 |
| Western Journal of Emergency Medicine | 1 |
