HealthPathways is an online decision support portal, primarily aimed at General Practitioners (GPs), that provides easy to access and up to date clinical, referral and resource pathways. It is free to access, with the intent of providing the right care, at the right place, at the right time. This case study focuses on the experience and learnings of a HealthPathways program in metropolitan Sydney during the COVID-19 pandemic. It reviews the team's program management responses and looks at key factors that have facilitated the spread and scale of HealthPathways.
Available data and experiences of two HealthPathways program managers were used to recount events and aspects influencing spread and scale.
The key factors for successful spread and scale are a coordinated response, the maturity of the HealthPathways program, having a single source of truth, high level governance, leadership, collaboration, flexible funding and ability to make local changes where required.
There are limited published articles on HealthPathways. The focus of spread and scale of HealthPathways during COVID-19 is unique.
Introduction
The first known cases of COVID-19 were reported in Sydney, Australia, in late January 2020 (ABC, 2020). At that stage, it was already apparent from overseas experiences that this was a major threat to the health and well-being of the population (Shamasunder et al., 2020; Douglas et al., 2020). This case study explores a single program's experience during COVID-19 in Sydney, Australia, in the state of New South Wales (NSW) in the context of wider NSW HealthPathways developments. Key insights are formed from two HealthPathways program managers' experiences.
In NSW, government-funded healthcare services are named Local Health Districts (LHDs). LHDs are responsible for providing hospital care and community health services for defined geographical areas (NSW Health, 2022). Primary care, such as that provided by a General Practitioner (GP), is completely separate to LHDs and primarily privately operated.
For the purpose of this case study the authors have adopted the European Union's Expert Group on Health Systems Performance Assessment's (2017, p 14) definition of Integrated Care:
Integrated care includes initiatives seeking to improve outcomes of care by overcoming issues of fragmentation through linkage or co-ordination of services of providers along the continuum of care.
There are no universally accepted definitions for spread and scale (Norton et al., 2012), so we defined scale as building up an existing program and defined spread as replicating an initiative somewhere else (Greenhalgh and Papoutsi, 2019). This can be as small as a pathway or as large as a new HealthPathways program. There can be overlap between these terms (Greenhalgh and Papoutsi, 2019).
HealthPathways has not been widely researched to date. Published studies tend to focus on implementation (Goddard-Nash et al., 2020). A recent systematic review of clinical pathway evaluations found limited studies specific to HealthPathways (Lee et al., 2019). The wider literature on clinical decision support tools show that they are widely used internationally; however, specific research on spread and scale of these tools is not apparent and needs to be inferred. For example, in a recent systematic review, Meunier (2023) focuses on barriers and facilitators to implementation of clinical decision support systems in primary care, these factors have the ability to influence spread and scale. The literature on spread and scale of integrated care initiatives is also lacking (Gordon et al., 2020; Maniatopoulos et al., 2020; Isaacksz, 2021).
This article focuses on program management functions; as such, we have not extended comment from other roles within the program. Program managers oversee all aspects of the program such as staffing, daily management tasks such as rostering, payments, decision-making, budgeting, leadership and drive the program to be efficient and effective. They also interact on a regular basis with program staff and stakeholders, as well as program managers from other HealthPathways programs. As a result of only using the experiences of the program managers, there may be biases or aspects that are not explored.
What are HealthPathways
HealthPathways is a community of programs that have exponentially grown in use since 2008 when it first started in Canterbury, New Zealand. Since that time, it has spread across New Zealand, Australia and the United Kingdom (Gray et al., 2018). Within NSW all but one region was covered by a HealthPathways program prior to the pandemic, this region received access during the pandemic. Now all of NSW is covered by 13 HealthPathways programs. In Australia, all 8 states and territories have HealthPathways programs; however, some areas within the states do not have a HealthPathways program. Internationally, there are nearly 50 health systems that have HealthPathways (Streamliners HealthPathways Community, 2023).
Each HealthPathways program is an online decision support tool, primarily aimed at GPs. Access is typically granted (at no cost to the user) to any local healthcare worker. In HealthPathways, the decision support helps GPs to assess, manage and refer based on up-to-date evidence-based information in the format of “pathways.” The pathways contain localised, concise, and pragmatic clinical information that can be used during a patient consultation. It also contains resources for patients and clinicians, local referral information and options for treatment. Having referral pathways in the same program as clinical pathways is what sets HealthPathways aside from many other decision support tools, as most only list clinical assessment and management.
Pathways are generally split into two main categories, clinical and referral pathways. The clinical pathways are designed to support a GP with a clinical presentation and are consistently structured in the format of background, assessment, management and referral. The idea is that a GP can work to the extent of their scope of practice through using the clinical pathway. The clinical pathway then guides the GP to use the referral pathway when the patient fulfils the criteria for referral. The referral pathways contain key information about local services (both public and private) including service specific criteria, contact details and any other useful information the GP might want to know when referring a patient.
Each pathway has an ability for users to provide feedback on the pathway's content to the HealthPathways program team; however, all aspects of a HealthPathways program, including requests for log in details, are asynchronous and rely on the program team opening an email in business hours and responding to it. McGeoch et al. (2015) described pathways in further detail, including images of a pathway.
It is important that the information in each HealthPathways program is developed collaboratively between local hospital Specialists and local GPs (Streamliners HealthPathways Community, 2023; Stokes et al., 2018). This process is called localisation or localising a pathway. The collaboration of local healthcare workers to develop the pathways ensures the pathways reflect how care is managed locally. A supplementary practical outcome of HealthPathways is that it forces discussion about what systems and referral pathways actually are, rather than what they are presumed to be, as well as highlighting gaps and unwarranted variations (Robinson et al., 2015). The GPs who write the pathways are paid for their work as part of the program team or as a consultant. When hospital-based subject matter experts (SMEs) provide feedback on the draft pathways, it is considered part of the SME's role and does not attract extra remuneration.
GPs are better supported to manage patients in Primary Care through the up-to-date clinical and referral information HealthPathways provides. The clinical advice is direct in guiding the clinician to the most appropriate level of care, helping the patient receive the right care, at the right place, at the right time. As a result, the hospital systems have the potential to receive higher quality, more complete and appropriate referrals. There is also potential to contribute towards reducing avoidable admissions and representations to emergency departments. To address community and socioeconomic factors, the HealthPathways team always list both public and private referral options so that GPs can help the patient find the most appropriate service. At present, there is limited empirical evidence published on HealthPathways to support these espoused values; however, wider literature on clinical pathways (including hospital-based care pathways) shows positive economic and health impacts. Also reported are reduced length of hospital stay, reductions in clinical process variation, decreased unnecessary procedures and adverse events (Lee et al., 2019).
Anecdotal evidence and ongoing funding of HealthPathways programs by LHDs and Primary Health Networks (PHNs) suggests that HealthPathways have support from their healthcare systems, and value is seen in its outcomes.
HealthPathways should be recognised as an integrated care initiative for multiple reasons including: collaborative multiorganisations partnership working; supporting seamless care for patients across primary and hospital care; and increasing workforce capability and capacity. This concept is explored in more detail later in the article.
Process for pathway development
Prior to the pandemic, HealthPathways programs were established in most areas of NSW. The NSW HealthPathways program teams regularly collaborated on work and shared ideas and knowledge. Sharing pathways has always been part of the culture of HealthPathways, but normally this involved using another region's pathway as a starting point. Then, the local team made as many changes as required to ensure all local stakeholders were happy with the content, ensuring it aligned with the local resources and ways of working. This process is termed “localising” a pathway.
Individual pathways within a HealthPathways program are generally developed in consultation between key stakeholders around a particular set of clinical conditions or service base. The development of pathways is undertaken by GP Clinical Editors who are local GPs skilled in, or with a strong interest in, medical writing. The clinical editor will collaborate with SMEs, who are relevant local hospital and community specialists, practitioners and occasionally peak bodies (e.g. Royal Australian College of General Practitioners and NSW Agency for Clinical Innovation) to ensure the pathway content suits both the needs of local primary care and the local hospital system. The focus is on accuracy, clarity and partnership development rather than haste.
There are considerable benefits of being able to localise pathways to an area's own context or share pathways unchanged when care is standardised across the state or country. Each pathway can cost hundreds or even thousands of dollars to develop. They are both time and resource demanding. The importance of being able to localise pathways means that they can be customised for how care occurs in the particular area they are being developed in. Some areas may have limited services and as such the pathway will need to help the GP work to an extended scope of practice, while in other areas, the GP may be instructed to refer to a specialist earlier in the disease trajectory as services have greater capacity. Other examples of localising to a context are when sharing pathways across states or countries, in this situation, there may be differences in guidelines or legislation necessitating changes to the pathway.
Prior to the pandemic, there were a few pathways that were identified as suitable for state-wide adoption where care had been standardised across the state, or there were only state-wide resources available which can make localisation unnecessary. Once developed by a NSW team, they would let the other teams know that they were available and the team would copy the pathway, make any changes if localisation was required and get local approvals. Traditionally, pathways were relatively static, being based on evidence and processes that did not change significantly in the short term. Their development was generally not a rapid process and most pathways only required routine review every 3 years.
What happened during COVID-19?
During the pandemic, information needed to get to GPs rapidly. As the health advice for COVID-19 care was changing frequently, the pathways also needed to be updated to align. Each change required review from high-level clinicians and officials who were already busy with pandemic responses. These clinicians would not have had capacity to continuously review sometimes daily updates to the required information. For a GP working in primary care, it would have been difficult to keep up to date with the constant changes in COVID-19 guidance, let alone any other conditions that a patient may present with. Throughout the pandemic, many GPs have attributed their ability to stay up to date with best clinical practice for COVID-19 to HealthPathways
For this to occur, a process needed to be created to enable these pathways to be developed collaboratively, while minimising the burden of information seeking. In addition, a process to make it easy to share the information with HealthPathways teams across the state needed to be implemented.
The NSW HealthPathways teams decided to work together to achieve an efficient and effective approach towards pathway development and ensure that GPs had reliable and accurate information throughout this time. Through a dedicated team working with high-level clinicians and officials, all the NSW HealthPathways teams were able to have available up-to-date information about anything a GP might need to know regarding COVID-19 assessment and management, including vaccinations.
At the start of the pandemic, GPs were not managing patients with COVID-19. Large COVID-19 testing centres were set up initially by NSW Health and later through private pathology providers. This meant that GPs generally continued with usual patient care. As the pandemic progressed, some GP practices started providing testing and management services. There were frequently changing criteria for what situations and who should be tested as well as extra testing centres opening up and closing down to ensure enough testing facilities were available in areas with outbreaks. All of this was regularly updated in the pathways.
When vaccinations became available, GPs were a key part of the response. Clinical vaccination pathways were developed and maintained by one NSW HealthPathways team for all of NSW. These vaccination pathways were constantly changing in line with emerging evidence to support GPs.
Major centres for vaccination were initially set up by NSW Health, not all GPs were providing vaccinations immediately. Once it became more common, there was little need to have the referral information (locations where patients can be vaccinated) in HealthPathways.
Method
This is a descriptive case study, discussing data available through various means to the program managers and uses the program managers' experiences. The case was chosen as it had interesting experiences worth sharing and because it was accessible.
Data were collected through structured meetings between the program managers, Google Analytics and a HealthPathways database.
The article focuses on the experiences and understandings of the program managers, which brings assumptions and biases. The program manager position interacts with all stakeholders and team members and is pivotal in project management aspects from planning to management and execution but may not be aware of every aspect that influences spread and scale of the program. This viewpoint has been chosen as the focus of the article is on program management functions. The program managers are the role that oversees all program functions and so are in the best position to comment. Other positions in the program such as sponsors, project officers, clinical editors and SMEs are not exposed to the detail and breadth we want to explore in this article and are intentionally not pursued. The small number of program managers included is appropriate for this case study; however, wider study of program manager experiences and other programs would be required to know if these findings are representative of more HealthPathways programs.
Shortcomings in the design and analysis are that both teams (case and comparator) are metropolitan teams in NSW, and this may have influenced the findings towards results that are only representative of metropolitan NSW programs. There may be different experiences rurally or in other states and countries.
As a retrospective piece, some of the subjective aspects may have biases due to recounting events rather than using accurate records taken contemporaneously. Having authors as subjects is a participant and researcher bias, however enables us to provide insights that would likely not have been achieved otherwise. Having two program managers involved has enabled comparisons, added validity to shared recollections and provided the ability to consider differences in perspectives.
Positionality
This research topic was chosen as a result of positionality of the lead author and their experience as a HealthPathways program manager during the pandemic. In terms of positionality, both program managers would be considered to have insider perspectives, being part of the community of HealthPathways programs for numerous years. Benefits of this positionality are that the program managers are already immersed in the program and have years of knowledge around how the program works, stakeholders and the organisations they are part of. This positionality enabled access to a comparison program and data, as well as participation of the second program manager. The two HealthPathways program managers' experiences have shaped this research and influenced what aspects are considered important to include in this study.
The lead author identifies as both a health manager with a clinical background and is undertaking a Doctor of Public Health (DrPH) and as such increasingly also identifies as a researcher. Two other authors identify as health managers with clinical backgrounds. The other three authors are academics. Four of the authors are also DrPH supervisors.
Findings and experiences were generated by reflection between the two HealthPathways managers, which confirmed similarities but also helped to highlight differing experiences. Having these positions inside HealthPathways management has enabled access to the experiences, as well as availably and understanding of the data. Reflexivity has also been strengthened through involving non-program managers and people not involved in HealthPathways in the research. This included experienced supervisors providing advice and feedback.
HealthPathways case study
This case study focuses on one of the 13 HealthPathways programs in NSW. The HealthPathways program (Program A) in this case study is located in a metropolitan area in Sydney, Australia. It was chosen as one of the authors manages the program and as such has valuable insights into the program management elements and identified that aspects of their experiences were worth sharing widely. A comparison between program A and an anonymous program, also in NSW at the start of the pandemic, is provided in Table 1. The comparative program is representative of a number of more mature HealthPathways programs in NSW as program maturity has an impact on experiences. It has been running longer but is located in a similar geographic area.
At the time of the first COVID-19 outbreak in Sydney, program A was approximately one and a half years old. There were 172 localised pathways and 191 different users per month.
In January 2020, the first pathway in response to the emerging pandemic, “Pandemic Respiratory Illness,” was developed by program A with input from lead clinical editors from other regions. This took place just as COVID-19 had started to spread to Australia. The pathway was subsequently used on 18 other HealthPathways sites.
As the threat continued to escalate, another well-established NSW team took the lead in developing most of the COVID-19-related pathways and keeping the information up to date as guidance changed. These COVID-19 pathways were developed with an all-of-state approach, so information was not location specific and was based on the NSW Health advice. Each team was responsible for keeping their local information about COVID testing centres up to date. The vendor company (Streamliners NZ) worked closely with the teams to ensure that the process of sharing these pathways was as easy as possible. As the pathways were being developed for the whole state, it became easier to get input from peak bodies, as they knew that input on pathways would help to get information to GPs state-wide.
As the pandemic progressed, more evidence emerged of some of the longer lasting effects of the virus. As a result, a different NSW HealthPathways program localised a “post COVID-19 conditions” pathway from a Victorian HealthPathways region for use across NSW teams. Another NSW HealthPathways program took the lead for vaccination pathways and kept these pathways up to date for NSW despite regular changes being required.
Individual HealthPathways teams had quite different experiences during this period. The differences observed and how the programs responded during the pandemic are interesting and are explored in terms of spread and scale.
Program A
Program A had been live less than two years when the pandemic broke out. It is a collaborative partnership between four organisations and spans a geographical area of over 450 square kilometres, servicing a population of over 900,000 residents. The partner that manages the program on behalf of the others has three major public hospitals and many other smaller hospitals and community health centres as part of its LHD. Two of the other partners both have a major metropolitan hospital, and the remaining partner is a PHN. There are over 1,100 GPs and GP registrars in this area.
At the start of the pandemic, program A analysed potential needs that might have to be met by the GP workforce if the pandemic progressed to the extent that had already been seen overseas. As program A was younger than many other NSW HealthPathways programs, there were key groups of pathways that had not yet been developed. The program stakeholders agreed it was essential to finish off all incomplete respiratory pathways to help with differential diagnosis and comorbid respiratory conditions. Additionally, it was identified that there were other key clinical areas that may become essential during the pandemic. These areas were mental health and palliative care. The team immediately started work to develop those pathways in addition to any work required to take the COVID-19 pathways developed by other teams.
To facilitate sharing of knowledge, pathways, and raise any issues, regular meetings between the NSW teams and the HealthPathways vendor occurred weekly at the emergence of the pandemic and first set of lockdowns in NSW. During this time, it was brought to the team's attention that in some areas, there was a noticeable increase in page views of domestic violence and abuse. For this reason, program A also developed these pathways as a priority.
Shortly after the first lockdown in NSW (31 March 2020), substantial supportive (8) COVID-19-specific pathways were live. By August 2021, there were 16. This included a combination of pathways developed by other teams and locally. All needed local approval before going live.
In total, program A developed over 70 pathways (excluding COVID-19) pathways specifically in response to the pandemic. Work on pathways that were already in development prior to the pandemic was continued concurrently, as able; however, priority was placed on the pandemic response pathways.
Peak usage of program A occurred when COVID-19 care was changed from hospital managed to managed by GPs. At this time, HealthPathways was intentionally chosen at the state level as the only place-specific information on COVID-19 for GPs would be made available as a single source of truth. Data showing program A's progress during this time are provided in Table 2. Usage data show considerably more GPs using the pathways during COVID-19 than prior to the pandemic. HealthPathways greatly assisted in getting accurate and up-to-date information rapidly out to many GPs. GPs could go to HealthPathways as their only source and know it was up to date.
The program manager is employed by the LHD, which provides easier access to clinicians and decision makers required to provide feedback on pathway development or pathway changes. Additionally, the program has supportive program sponsors from each partner organisation and is supported through leaders in the other NSW HealthPathways teams working collaboratively towards the same goal.
Program comparison
At the time of the pandemic, many other NSW HealthPathways programs had already developed key pathways such as mental health, palliative care, domestic violence and respiratory. The programs which already had these pathways were able to continue to focus on adopting the COVID-19 pathways developed by other regions, developing lead region pathways, continuing some of their business as usual, as well as some were able to help their LHD with the public health response.
Findings
High-level governance, collaboration and improvement
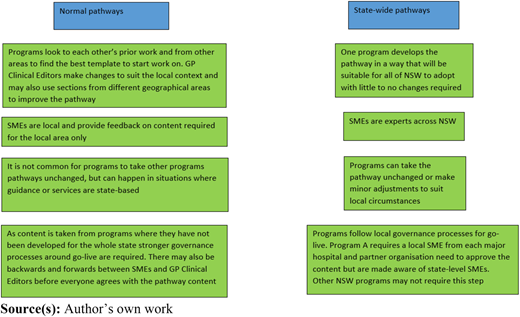
The pandemic brought about a need for sharing of the pathway development workload in a timely and efficient way. To expedite efficient development and maintenance of COVID-19-specific pathway content, a model of state-wide and lead-region pathways were developed allowing programs to take the pathways unchanged or make small localised changes. The pathways are developed by a team nominated to develop the pathway for the state, and for state-wide pathways using SMEs with a state remit ensures state-level governance and provides assurance that the pathway is suitable for all NSW teams. This enabled a single source of truth that other HealthPathways regions would utilise with none to minimal change. This sharing methodology has created a far more efficient process for HealthPathways teams to share their work going forwards (Figure 1). The collaborative allocation of tasks across the NSW teams, due to the collaborative governance, also resulted in efficiencies.
The vendor company facilitates spread and scale through ensuring consistent layouts, wording, governance, providing user data and a dedicated resource to facilitate pathway sharing. This assists with the spread of pathways across teams. There are strict rules about not publishing clinical pathways if corresponding referral information is not already developed. Due to this rule, some of the younger teams with less referral content encountered barriers, experiencing difficulty taking pathways identified as useful for spreading across NSW because they did not have some of the required referral links. Teams are now more aware of how to set up pathways to facilitate all teams to be able to take the pathways faster and easier. This is particularly important for a new program which was set up during the pandemic to support local GPs. As a new team, they did not have any other pathways, so it was important that state-wide pathways were developed with teams such as them in mind.
An example of barriers faced taking on state pathways is the post-COVID conditions pathway which was developed early in the pandemic. Program A had extensive delays in adopting this pathway because they were unable to localise some of the referral pathways that were not priority areas for development.
The newer COVID pathways designed for the state tend to include drop downs of pertinent points or useful links to websites, rather than reliance on existing pathway material. They also use sections for local information, with the remaining information updated at a state level. This ensures the pathways suit local context as well as LHDs with differing needs and services.
Funding and sustainability
The sustainability of individual pathways is generally not resource intensive. After a pathway is developed, all of the stakeholders agree to a timeframe that is suitable to review the pathway. This may be short if it is an area of frequent change, up to a maximum of three years for areas unlikely to change. At that point, all editors and relevant SMEs review the pathway in question and decide if it needs to be updated. This ensures that the program stays up to date and relevant, so that GPs continue to use the program.
During COVID-19, some of the pathways developed required a lot of resources due to the frequent changes in health advice to align with state and federal guidelines. For this reason, pathways such as the COVID-19 vaccination pathways are not at all sustainable and providing the frequent updates in line with changes to the vaccination guidelines would have taken away from the team's ability to conduct business as usual. For the teams using the pathway, not having up to 12 other teams researching and updating, this information is a large efficiency despite all teams needing to locally check the updates.
Some teams would not have the budget to be able to develop these state pathways, let alone keep the content up to date. Financial support for the teams developing these pathways was discussed multiple times; however, for most teams, this did not eventuate until the team developing the vaccination pathways was able to secure dedicated funding from the state funding body to keep the pathways up to date. There was still a significant amount of resources required by each team when adopting the COVID-19 pathways, even though they are optimised for sharing.
HealthPathways partnerships can find it difficult to fund these programs especially when a significant increase in workload is required, as generally HealthPathways programs are only sustainable through the local partners' financial contributions. Although there are assumptions that use of HealthPathways could lead to a reduction of unnecessary specialist appointments and emergency department presentations, there is no clear evidence that this occurs. The programs are completely dependent on partners seeing value in the work, as proving a reduction in hospital attendances is almost impossible without resource intensive properly designed research.
Factors for achieving scale
A major factor influencing the different “spread and scale-up” responses required appears to be the length of time the program has operated. As program A was younger than many other programs, there was a much larger workload required during this period of time to get the necessary pathways live.
In the HealthPathways context, we defined scale as building up an existing program.
Examples of scaling are developing more pathways within an existing program and achieving more use of the pathways.
Perceived facilitators for achieving scale in HealthPathways programs are as follows:
Sharing the workload
High-level governance for quick ability for all teams to take up pathways
Burning platform – pandemic
Existing strong relationships, structures and trust
Leadership
Barriers were as follows:
Resourcing (financial, time and staffing)
Governance processes and level of engagement required
Being a younger program (less existing content to link to)
Factors for achieving spread
In the HealthPathways context, we defined spread as replicating an initiative somewhere else (Greenhalgh and Papoutsi, 2019).
Examples of spread include starting a new HealthPathways program but can also be as small as the individual pathway level. Whether a pathway has spread or scaled depends on the perspective of the team. If a team is localising a pathway that another team developed, then they are scaling up their program. From the perspective of the team who originally developed the pathway, this would be seen as spread of the pathway.
Perceived facilitators for spread in HealthPathways programs include the following:
Flexible funding arrangements and high-level support
Ability to rapidly change
Ability to suit local context
Leadership
Trust
Barriers were the same as for scale.
The facilitators and barriers for spread and scale of HealthPathways cover comparable categories to those of Meunier's (2023) systematic review of “barriers and facilitators to the use of clinical decision support systems in primary care”, which were categorised into human factors, organisational factors, technological factors and net benefits.
During this period of time, the remaining area in NSW without a HealthPathways program was able to be set up with access to the COVID-19 pathways faster than any other program in NSW had been. This could not have happened if this system for rapid sharing and updating of pathways had not been developed.
How HealthPathways fits into integrated care
HealthPathways fits within integrated care for multiple reasons:
Patient at the centre of care, with the aim of providing the right care, at the right place, at the right time
Partnership working, with collaborative governance and funding arrangements
Formalises and improves referral pathways between primary, specialist and hospital services
Aims to meet the needs of population health
Supports GPs to work to the extent of their scope of practice
Collaboration across clinicians who might not usually be in communication, allowing time and space to discuss how care and services could be improved for patients in the area
During the COVID-19 pandemic, the International Foundation for Integrated Care (IFIC) released a document exploring a conceptual framework for successful integrated care implementation (IFIC, 2020).
The findings are explained using the building blocks of the framework to describe the HealthPathways COVID-19 experience and identify potential enablers to facilitate spread and scale of the pathways.
Shared values and vision
During the pandemic, it was clear to the already collaborative NSW HealthPathways teams that they needed to support each other with COVID-19 pathway development and that regular updates to these pathways would be required as information changed. All teams were keen to work together and benefit from each other's support and information arising.
Population health and local context
The pathways are always appropriate for the local context, and this is achieved by having local GPs and SMEs review the content and provide specific feedback with regards to how care should look in the local area.
Pathway development can be prioritised to meet population health needs. For example, during the pandemic, the priority focus was ensuring there was supportive COVID-19 content.
When developing the COVID-19-related pathways, there was always the need to provide plenty of options for primary care and community care in case the hospital systems became overloaded as had occurred overseas.
People as partners in care
The HealthPathways teams have clear feedback loops to enable anyone (especially local clinicians) to provide feedback to the team in charge of the pathway, so they could make any changes suggested by the users.
The pathways are developed as collaboration between local GPs and the local Health system, so they have representation from all stakeholders. The pathways enable GPs to support patients to make informed choices in their care, where appropriate.
Resilient communities and new alliances
New alliances were formed
A new Streamliners pathway sharing position was developed to facilitate sharing of pathways. A new regional NSW HealthPathways team was developed for the one (large) area not yet covered by a HealthPathways team. The state and national funding bodies recognised the impact of HealthPathways and started discussions about how to assist with funding the programs.
Resilient communities
HealthPathways programs are part of a community of practice and learning. They supported each other as the task of developing and keeping all the pathways up to date individually would have been impossible.
Workforce capacity and capability
The staff working on the HealthPathways program are all highly capable. Capacity to assist the public health response to COVID-19 outside of HealthPathways was dependent on the maturity of the program. Early in the pandemic, program A was very busy with HealthPathways development for the key areas that might be needed later in the pandemic, whereas other programs which had already developed these key pathways were able to support non-HealthPathways-related COVID functions required of their organisation, as well as developing lead region HealthPathways. In later waves, program A was also able to support the public health unit with contact tracing.
System-wide governance and leadership
Program A had supportive sponsors from all partners.
In addition, the extended team contains members with clinical and leadership backgrounds.
The wider group of NSW HealthPathways teams, with vendor support, collaborated to determine the level of governance required to develop state-wide pathways in a manner that was suitable for all teams but not overly time-consuming.
Digital solutions
HealthPathways is a digital solution to support GPs when they need it.
The vendor company created a secure shared spreadsheet to assist teams with knowing which pathways were available for sharing. Jointly, a process was developed to ensure that teams had all of the information they needed to take a pathway from another region and decide if they wanted to receive automatic updates as the lead team updated the pathway or just to receive notifications of the changes so that they could make local decisions whether to update their pathway as a result.
Aligned payment systems
Each team has their own pre-arranged funding arrangements between partners.
The work developed by individual teams on COVID pathways was not evenly distributed or funded, and it occurred through teams nominating themselves. The teams that took on the work were not compensated by NSW Health or the Australian Government until negotiations occurred mid-way through the vaccination pathways.
There is interest from the peak funding bodies to assist all of the HealthPathways programs financially. Both state and national funding bodies are committed to the ongoing use of HealthPathways as a support platform for primary care. As per other jurisdictions in Australia, funding and resourcing is being considered.
Transparency of progress, results and impact
Transparency is very important for program A, which report on progress, results and impact at least monthly to all partners. Data are available to the program managers on pathway development through the vendor's system. Data on usage of the pathways have been made available to the program managers by the vendor through Google Analytics.
Discussion
Leadership, flexibility of prior plans and funding, and supportive partners are all important factors that have facilitated spread and scale in program A and likely more widely across NSW HealthPathways programs.
Spread and scale has been facilitated by practices used by the vendor company and through the collaboration between the NSW teams. The NSW teams themselves facilitated spread and scale through regular meetings and relationships that enabled teams to share information, pathways and practices that were working in their areas so that other teams could consider localising the initiative.
The speed and scale of the response was increased through regular NSW-wide COVID/pathway sharing meetings and information was shared between the vendor and across all HealthPathways teams. The state and national approaches to the pandemic enabled pathway development to be centralised, using a lead region to develop and maintain pathways, with ability to spread the pathways across the state in mind.
Generally, programs that had been in place longer were more able to take up lead region roles as younger programs had other important pandemic related pathways to develop. All teams needed to be flexible and adjust their plans to ensure the new COVID pathways could be added to their program in a timely manner.
It is important that the wider HealthPathways community continue to use these spread and scale learnings in business as usual. Key aspects such as using the new pathway sharing model and regular state-wide meetings between team leads and the vendor company will help deliver the program efficiently and effectively, which in turn supports GPs and the hospital system. Ongoing improvements should continue to take place to optimise this process both at the state level and in individual programs.
More HealthPathways programs and integrated care programs need to publish on spread and scale, regardless of whether the initiative is successful or fails. This will help managers and policy makers make informed decisions when trying to spread and scale initiatives.
Lessons learnt
Leadership, flexible funding arrangements and supportive partners are essential.
Project maturity had a large impact on the required responses of HealthPathways programs.
Flexibility of prior plans to allow for new high priority pathways to be localised.
Sharing/spread/scale required a collaborative effort and ongoing improvement work to optimise the processes.
Limitations
Two authors are program managers from two different NSW HealthPathways teams, one being program A. This brings benefits and biases to the paper.
Only studying one program and two program managers means there is a small sample size. As a descriptive piece, it can be said that many aspects are opinions and may be subjective. A larger piece of work is needed to determine if these are also the views of the wider NSW HealthPathways teams, especially considering both managers are located in metropolitan areas. As a result, this may not be reflective of all the experiences, barriers and enablers faced by other programs.
Conclusion
Processes can be optimised to facilitate spread and scale of integrated care initiatives. The key factors for spread and scale are a coordinated response, the maturity of the HealthPathways program, having a single source of truth, high-level governance, leadership, collaboration, flexible funding and ability to make local changes where required.
Each HealthPathways program had a different response during the pandemic. They achieved what was required through leadership, flexibility, working collaboratively and having to think about improving the process to facilitate spread and scale at a time where everyone was extremely busy with pandemic responses.
It is essential that the HealthPathways community continues the new collaborative practices brought about by the pandemic to ensure efficient and effective pathways development and delivery and embed quality improvement into the program. We also encourage more research and publication within the HealthPathways community. Areas for future research should include detailed requirements to develop new pathways in comparison to using the other pathway-sharing methods, barriers and facilitators to use of HealthPathways, as well as a larger study incorporating all of the NSW programs to understand if they had the same experiences during COVID around spread and scale.
This paper forms part of a special section “Exploring the Expansive Horizons of Integrated Care”, guest edited by Dr Axel Kaehne.
Anna McGlynn is supported through an Australian Government Research Training Program Scholarship.