

The purpose of this study is to summarize the available pool of literature on service quality to identify different dimensions of service quality in the healthcare industry and understand how it is measured. The study attempts to explore the research gaps in the literature about different service quality dimensions and patient satisfaction.
A systematic literature review process was followed to achieve the objectives of the study. Various inclusion and exclusion criteria were used to select relevant research articles from 2000–2020 for the study, and a total of 100 research articles were selected.
The study identified 41 different dimensions of healthcare service quality measurement and classified these dimensions into four categories, namely servicescape, personnel, hospital administration and patients. It can be concluded that SERVQUAL is the most widely used service quality measurement tool.
The study identified that a majority of the researchers deduced a positive relationship between SERVQUAL dimensions and the quality of healthcare services. The findings of study will assist hospital executives in formulating effective strategies to ensure that patients receive superior quality healthcare services.
Introduction
The quality of healthcare services has long been a subject of concern for both private and public healthcare service providers across the globe. According to Senic and Marinkovic (2013), integrity and competitiveness of a nation's healthcare structure are gauged by the quality of healthcare services rendered. Indian National Health Policy 2017 envisions that everyone should have access to high-quality healthcare without facing financial suffering (MoHFW, 2017). Adherence to quality standards and improved quality design results in a better-perceived value, which leads to better prices, better income and greater profitability (Zeithaml, 2000). Customers of the healthcare industry in developing countries are becoming more and more aware of their right to quality healthcare. Consequently, delivering high-quality service by healthcare service providers is gaining momentum (Abuosi & Atinga, 2013). According to Yee, Yeung, and Cheng (2010), healthcare service providers need to provide high-quality services to sustain the trustworthiness of patients. Demand for superior service quality is growing due to an increase in the per capita income of customers and increased aspirations of the customer (Singh & Prasher, 2019). Also, as a result of competition from private healthcare service providers, public care providers are facing pressing demand for delivering high-quality services (Zarei, Arab, Froushani, Rashidian, & Ghazi-Tabatabaei, 2012).
Mosadeghrad (2014, p. 78) defined healthcare quality as “consistently delighting the patient by providing efficacious, effective and efficient healthcare services according to the latest clinical guidelines and standards, which meet the patient's needs and satisfies providers”. Ovretveit (2009, p. 4) defines quality care as the “provision of care that exceeds patient expectations and achieves the highest possible clinical outcomes with the resources available”. Parasuraman, Zeithaml and Berry (1985) described service quality as the gap between a customer's expectations of service and the customer's perception of service after the service is rendered. When perception exceeds expectations, the customer will be satisfied (Kalaja, Myshketa, & Scalera, 2016). Several studies have confirmed that customer expectations of service are much higher than the customer perception of services rendered by both public and private sector institutions (Andaleeb, Siddiqui, & Khandakar, 2007; Zarei et al., 2012; Manulik, Rosińczuk, & Karniej, 2016). A firm provides quality service when its services at least meet or exceed the expectations of the customer (Owusu-Frimpong, Nwankwo, & Dason, 2010). Service quality evaluation varies from the service provider's and service receiver's point of view. Service delivery professionals evaluate service based on delivery and design aspects, while receivers of service evaluate it based on their overall perception after consuming the service (Brown & Swartz, 1989). Traditionally healthcare quality was judged based on some objective criteria such as mortality rate, morbidity rate, infant mortality rate, etc. However, as time passes, the structure of the industry changed, and the role of patients in deciding quality has been given more and more consideration (Dagger, Sweeney, & Johnson, 2007). To survive in the modern competitive markets, it has become of utmost importance for service providers to understand the needs and expectations of customers. They must deliver what the customer is expected instead of what they feel is important for a customer to maintain the business demand (Singh & Prasher, 2019). Kotler and Keller (2006) suggest that in the consumer-oriented healthcare market where healthcare delivery is commodified and patient-led, the patient should be the judge of service quality. Hence, to provide better quality services, healthcare service providers need to identify the main dimensions of service quality in healthcare and focus on those dimensions rated more important by the patients (Singh & Prasher, 2019).
Studies on healthcare service quality have been conducted in a variety of settings worldwide, namely Albania (Kalaja et al., 2016), Australia (Copnell et al., 2009; Dagger et al., 2007; Levesque & Sutherland, 2020), Bangladesh (Andaleeb et al., 2007), China (Li et al., 2015; Wu, Li, & Li, 2016), Denmark (Engelbrecht, 2005; Groene, Skau, & Frølich, 2008), Ghana (Abuosi & Atinga, 2013; Agyapong, Afi, & Kwateng, 2018), India (Chahal, 2008; Aagja & Garg, 2010; Chahal & Kumari, 2010; Gupta & Rokade, 2016; Singh & Prasher, 2019; Upadhyai, Jain, Roy, & Pant, 2019; Jog et al., 2020), Iran (Goshtasebi et al., 2009; Mohammadkarim, Jamil, Pejman, Seyyed, & Mostafa, 2011; Mosadeghrad, 2014), Malaysia (Ahmad & Sungip, 2008; Hasan, Ilias, Rahman, & Razak, 2009), Pakistan (Irfan & Ijaz, 2011; Shabbir, Malik, & Malik, 2016; Fatima, Malik, & Shabbir, 2018; Dhahri, Iqbal, & Khan, 2020), Turkey (Beyan & Baykal, 2012) and USA (Lee, 2003; Hegji & Self, 2009; Mustafa, Yang, Mortezavi, Vadamalai, & Ramsey, 2020; Thompson, Shen, & Lee, 2020). The purpose of this paper is to investigate and summarize the available literature on healthcare service quality to understand what constitutes healthcare service quality and its principal dimensions and also to highlight the prominent research gaps that will provide direction for future research.
Methodology
The study followed a systematic review process to obtain research articles relevant to the research problem understudy. The systematic review process is a structured way of identifying, evaluating and interpreting the available literature related to any particular area (Kamboj & Rahman, 2015). A systematic literature review is a two-step process. First, defining the criteria for inclusion of articles and second, identifying databases and research studies (McLean & Antony, 2014).
Inclusion criteria
Papers published during 2000–2020 were considered for the study. This was done by applying a custom range filter. The reason for selecting the above mention time frame is the most recent two decades were selected for article search.
Research articles related to healthcare service quality were included in the review process. The criterion was adopted in line with the primary objective of the review process.
Empirical and review articles published in peer-reviewed journals were considered.
Only papers in the English language were included.
Database and article selection
The literature search was conducted in the autumn of 2021. The databases selected for the literature search included Emerald, Elsevier, Sage, Taylor and Francis and Google Scholar. Filters such as custom range and sort by relevance were applied to restrict the search results to keywords. The systematic review process is presented in Figure 1. In stage 1 of the review process, the literature was searched using the keywords such as healthcare, healthcare services, service quality and SERVQUAL. The search obtained 209 research articles. The research papers were selected based on relevance to the topic understudy and the popularity of the articles. Researchers such as Beaulieu (2015) argued that the popularity of journal articles with above 10 citations are considered in top 24% of the highest cited articles, and articles that receive 100 citations are considered among 1.8% of the most popular articles across the globe, which makes the current study a worth addition to the existing body of literature. In stage 2, the screening of articles was then conducted first based on title and abstract and then based on inclusion criteria. Screening of articles based on the title and abstract resulted in the exclusion of 63 research articles, and 146 articles were moved to the next level of screening.
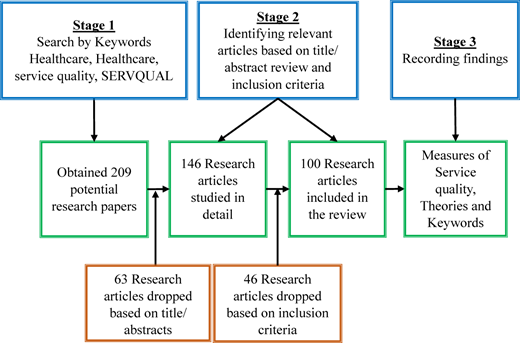
Then articles were screened by applying inclusion criteria to exclude articles that do not fulfill the above-stated criteria (Kamboj & Rahman, 2015). This screening obtained 100 research articles that were finally considered for review, and the rest of the articles (46) were excluded from the study. Finally, in stage 3 of the review process, the study provides a summary (publication trend, journal-wise distribution, methodology that includes sampling method and data analysis tools used and key findings) of the 100 articles included in the review.
Common characteristics of reviewed articles
Classification of articles by research type and hospital setting
Table 1 displays the classification of research articles based on research type and hospital setting. The research type describes the nature of the research and yields that a maximum number of articles were quantitative studies (62 articles) followed by qualitative studies (15 articles) and only 07 studies that were both qualitative and quantitative. A few review articles (14 articles) were also considered during the process. The results of the review substantiate that there is a need of conducting qualitative research that can provide an in-depth understanding of how various service quality dimensions affect the perceived quality of care among patients and the treatment satisfaction level. Qualitative studies can also provide insights into the priorities of patients while receiving medical services.
Classification of articles by research type and hospital setting
The classification based on hospital setting yields more than 77 articles that have purposively chosen a specific hospital setting and the rest have collected data from respondents in general. Out of 77 articles, 49% of research studies were conducted in a public hospital setting, and 25% were conducted in a private hospital setting. Around 26% of research were conducted in both public and private hospital settings. The direct comparison of healthcare services and perceived service quality among patients was observed as the main motivator in choosing both hospital settings (Ovretveit, 2000; Mostafa, 2005; Taner & Antony, 2006; Andaleeb et al., 2007; Owusu-Frimpong et al., 2010; Manulik et al., 2016; Dhahri et al., 2020).
Data analysis tool
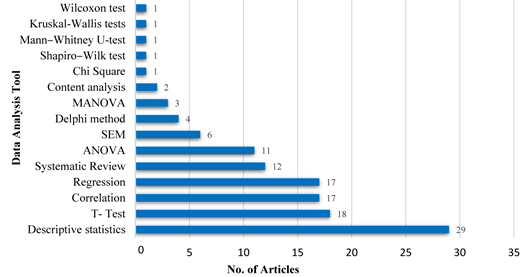
Figure 2 presents the frequency of various data analysis tools used by researchers to obtain meaningful results. The examination of articles selected for review revealed that 15 different data analysis techniques have been utilized in the past two decades. Descriptive statistics (29 articles) including mean and standard deviation has been the most frequently applied technique in healthcare service quality research followed by t-test (18 articles). It was also found that both techniques have been applied in combination because service quality can be obtained by ascertaining the difference between service perception and service expectation of patients using the SERVQUAL model (Ahmad & Sungip, 2008; Irfan & Ijaz, 2011; Zarei, Daneshkohan, Khabiri, & Arab, 2015; Torabipour, Sayaf, Salehi, & Ghasemzadeh, 2016). Other major techniques preferred by researchers include correlation (17 articles), regression (17 articles), systematic literature review (12 articles) and ANOVA (11 articles). However, only 20 articles in total have applied structural equation modeling (SEM), MANOVA, content analysis, chi-square test, Shapiro–Wilk test, Mann–Whitney U-test, Kruskal–Wallis tests and Wilcoxon test, making them among the least preferred techniques in healthcare service quality research.
Sampling method
Articles selected for review depict that both nonprobability and probability sampling have been applied to study healthcare service quality and patient satisfaction. The articles have adopted 08 different sampling methods in addition to the complete enumeration (Census), which was employed for 03 articles. From nonprobability sampling techniques, convenience sampling (18 articles) is the most widely used sampling technique, and simple random sampling (19 articles) is the most frequently applied sampling method from the probability sampling group. Cluster sampling was found to be the least applied sampling technique among probability sampling methods because most of the studies were focused on specific regions with a limited geographical area. Targeting a smaller geographical area or specific site increases the feasibility of reaching out to sampling units because of the limited population spread. Therefore, when further segregation based on the geographical area seems impossible, the applicability of cluster sampling becomes impractical (Cameron & Miller, 2015).
Findings and discussion
The systematic review of 100 articles has fetched several important findings in terms of measures of healthcare service quality and the theories applied in examining healthcare service quality.
Measures of healthcare service quality
Healthcare service quality, because of its intangible character and subjective nature, is difficult to define and measure. The comprehensive study of research articles about healthcare service quality illustrated that service quality in healthcare is examined by using different measures primarily related to servicescape, personnel, hospital administration and patients. The study has identified 41 distinctive measures of healthcare service quality (Table 2). The factors commonly used to measure the quality of servicescape are identified as physical environmental quality, diagnostic aspect of care, resources and capacity, tangibility, financial and physical access to care and access (Herstein & Gamliel, 2006; Ahmad & Sungip, 2008; Sharma & Narang, 2011; Simou, Pliatsika, Koutsogeorgou, & Roumeliotou, 2014; Marzban, Najafi, Etedal, Moradi, & Rajaee, 2015). Among the mentioned dimensions of servicescape, utilization has been less studied in the past. Future researchers can explore these areas because often in healthcare centers, the infrastructure capacity is overutilized or underutilized, which hinders the delivery of healthcare services. The determinants mostly employed to determine the quality of human resources (personnel) include healthcare personnel conduct, efficacy, efficiency, empathy, interaction quality, physician and staff performance, provider competency/performance, reliability, responsiveness, timeliness and trustworthiness (Chahal & Kumari, 2012; Manulik et al., 2016; Singh & Prasher, 2019). Some of the fewer studied factors under personnel characteristics include quality of patient-staff communication, outcome quality, professional quality, provider motivation and satisfaction encounters. These factors can influence the service quality of healthcare centers but are less researched in the past. The factors concerning quality aspects of hospital management/administration include admission, assurance, healthcare delivery system, infection rate, standard operating procedures, leadership and management and medical service (Ovretveit, 2000; Herstein & Gamliel, 2006; Taner & Antony, 2006; Aagja & Garg, 2010; Irfan & Ijaz, 2011; Gupta & Rokade, 2016; Torabipour et al., 2016). Among the determinants of hospital administration availability of doctors and paramedical staff, discharge mechanism of patients, documentation procedure in the hospital, social responsibility consciousness among the staff, management quality and drug availability in the hospital are some of the key factors that influence the service encounters between staff and patients. These determinants are less studied in the literature. Future researchers can build their research on these less studied variables. Lastly, the factors affecting service quality in terms of patient characteristics include patient satisfaction, the average length of stay, patient cooperation, patient quality/illness and patient socio-demographic variables (Ovretveit, 2000; Mosadeghrad, 2014; Gupta & Rokade, 2016). It was observed that most of the service quality determinants identified can be summarized under the major 05 SERVQUAL determinants.
Measures of healthcare service quality
Theories applied to healthcare service quality
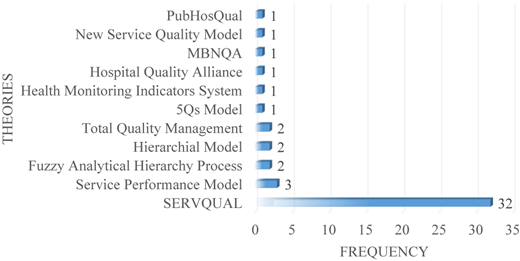
The list of popular theories that have been applied to examine healthcare service quality across the globe is presented in Figure 3. A total of 11 different theories were identified during the review process. Less than 50% of papers identified for review have adopted one or the other service quality measurement framework and around 70% (32 research articles) among them have applied the SERVQUAL framework by Parasuraman, Zeithaml, and Berry (1988). This makes SERVQUAL the mostly widely applied service quality framework. The other theories that have been utilized in the recent decade to examine the service quality of healthcare system include total quality management, fuzzy analytical hierarchy process, service performance model and health monitoring indicators system: health map (Chahal & Kumari, 2012; Ramez, 2012; Zarei et al., 2015; Amole, Oyatoye, & Adebiyi, 2015; Singh & Prasher, 2019; Zaid, Arqawi, Mwais, Al Shobaki, & Abu-Naser, 2020). The elements used to measure the perceived service quality of hospitals under different theories other than the SERVQUAL model can largely be classified under five SERVQUAL dimensions. However, outcome quality, process quality, administrative/management quality, utilization, technical quality and trustworthiness are identified as additional new dimensions being used to examine the service quality of hospitals (Ovretveit, 2000; Chahal & Kumari, 2010; Simou et al., 2014; Singh & Prasher, 2019; Zaid et al., 2020).
Limitations and future research directions
The current study has some shortcomings which open up opportunities for future research. The present study followed a systematic review process to obtain research articles from different databases, like Emerald, Elsevier, Sage, Taylor and Francis and Google Scholar. Several inclusion criteria were applied, and only those full-text articles that are available in the English language were selected for the review. Therefore, there is the possibility of excluding some articles that are not available in these databases or are available in some other languages. Further, most of the studies selected for review were from developed nations. There is a lot of difference between the healthcare system of developed and developing nations. Thus, the findings of the present study cannot be generalized to developing nations without additional validation (Kamboj & Rahman, 2015). Therefore, there is a need of carrying out empirical research in developing nations in this area.
The review of available literature has revealed that there are a large number of measurement tools available for the assessment of service quality in healthcare. However, the majority of these measurement instruments developed by the researchers assess quality from patients' perspectives and do not take into consideration service providers' perspectives. The technical aspect of service quality cannot be assessed by patients alone (Upadhyai et al., 2019). For a better understanding of service quality evaluation and satisfaction of service encounters, both service providers' and receivers' perspectives should be taken into consideration (Brown & Swartz, 1989). Therefore, future researchers need to explore the knowledge gap (gap 1) of the SERVQUAL gap given proposed by Parasuraman et al. (1985).
Practical implications
The study has attempted to identify and describe all dimensions and measurement tools relevant to healthcare service quality in light of the available literature. The study provides a thorough description of a vast number of investigations and reflects their outcomes. This research could help understand the diverse conceptualizations of service quality in healthcare compared to other types of services. The study also identified various gaps in the available literature that could be answered by future research.
The results of this study will help hospital executives in understanding the various constituents of quality and their impact on patient satisfaction. This will help hospital managers in formulating strategies that will improve patient satisfaction and ultimately improving the overall performance of hospitals. The study also highlighted the factors in which patients weigh more, thereby helping hospital managers to set priorities and help in proper resource utilization.
Conclusion
The current study presents an in-depth review of the literature concerning service quality and patient satisfaction in the healthcare industry. Service quality is a subjective measure and hence tends to vary from place to place and from patient to patient based on preference. The study has identified different measures that have been utilized to date to examine service quality or quality gaps in various hospital settings. Most of the studies selected for review have employed SERVQUAL dimensions of quality as service quality parameters. Service quality in the majority of the studies was established based on a difference between perceived and expected scores of service quality determinants, and the t-test was identified as the widely used statistical measure for testing its significance. In addition to this, various measures to determine patient satisfaction were identified and classified based on extra 3Ps of services marketing, namely physical evidence, people and process. The maximum number and most weighted factors affecting patient satisfaction are related to human resources actively engaged in providing medical services. It was observed that SERVQUAL determinants are popularly being used as a tool to determine the level of satisfaction among patients. All SERVQUAL determinants were found to have a significant positive relationship with patient satisfaction. Finally, 11 popular theories were identified among which SERVQUAL is widely applied.
 Dr Mushtaq Ahmad Darzi is Professor in the Department of Management Studies, University of Kashmir, Srinagar. His research areas are business financial management, portfolio management, accounts, social marketing, e-retailing and customer relationship management (CRM).
Dr Mushtaq Ahmad Darzi is Professor in the Department of Management Studies, University of Kashmir, Srinagar. His research areas are business financial management, portfolio management, accounts, social marketing, e-retailing and customer relationship management (CRM).
 Sheikh Basharul Islam is a research scholar at Department of Management Studies, University of Kashmir, Srinagar. His research interests include retailing, sustainable development, e-commerce and healthcare service quality.
Sheikh Basharul Islam is a research scholar at Department of Management Studies, University of Kashmir, Srinagar. His research interests include retailing, sustainable development, e-commerce and healthcare service quality.
 Syed Owais Khursheed is a research scholar at Department of Management Studies, University of Kashmir, Srinagar. His research interests include horticulture finance, rural marketing and consumer behavior.
Syed Owais Khursheed is a research scholar at Department of Management Studies, University of Kashmir, Srinagar. His research interests include horticulture finance, rural marketing and consumer behavior.
 Dr Suhail Ahmad Bhat is a faculty at the Department of Management Studies, University of Kashmir, Srinagar. His research interests include e-marketing, green marketing, social marketing, sustainable development, CRM and different facets of CRM in the service industry. He has published papers in national and international journals such as International Journal of Bank Marketing, Vikalpa, Decision, Global Knowledge, Memory and Communication, Vision, International Journal of Tourism Cities, South Asian Journal of Business Studies, FIIB Business Review, Paradigm, Pacific Business Review International, Abhigyan and Productivity.
Dr Suhail Ahmad Bhat is a faculty at the Department of Management Studies, University of Kashmir, Srinagar. His research interests include e-marketing, green marketing, social marketing, sustainable development, CRM and different facets of CRM in the service industry. He has published papers in national and international journals such as International Journal of Bank Marketing, Vikalpa, Decision, Global Knowledge, Memory and Communication, Vision, International Journal of Tourism Cities, South Asian Journal of Business Studies, FIIB Business Review, Paradigm, Pacific Business Review International, Abhigyan and Productivity.
