The purpose of this study is to explore how the COVID-19 pandemic, and related preventative measures, impact global stressors on autistic children, adolescents and their families.
This exploratory study compared two cohorts, one spanning just before and throughout the pandemic, and one during a non-pandemic period, to explore child functioning and parenting stress in families with autistic children. Autism symptom development was assessed using the Social Responsiveness Scale-2 at three-time points, while emotional and behavioral functioning was examined across two-time points using the Brief Problem Monitor. Parenting stress was assessed using the Parenting Stress Questionnaire.
Results indicated no significant differences between the cohorts in parent-reported autism symptoms or the emotional and behavioral functioning of autistic children and adolescents. Whereas no differences emerged in children’s functioning, during the COVID-19 pandemic period parents reported more parental role restriction and physical health problems along with fewer parenting problems compared to parents during a non-pandemic period.
These findings provide insight into how families were potentially influenced by the COVID-19 pandemic. It seems that parents in particular may benefit from more tailored support, such as flexible respite services, remote interventions and self-care programming designed for parents of autistic children, especially in times like a pandemic.
The COVID-19 pandemic brought significant change to daily life, including safety measures of social distancing, mask mandates and quarantines. In 2021, the Netherlands reported 60,000 hospitalizations and 19,400 deaths due to COVID-19 [National Institute for Public Health and the Environment of The Netherlands (RIVM), 2022]. However, for most, the pandemic’s repercussions were felt in daily life through school and business closures, limited social gatherings, and reduced access to specialized treatment [National Institute for Public Health and the Environment of The Netherlands (RIVM), 2022]. For families, this often meant adapting to remote work and education, relying on household or virtual support and managing increased caregiving demands. Understanding the pandemic’s influence on child functioning and family functioning, particularly among families with children with autism spectrum disorder (ASD), is essential for ensuring appropriate supports and services are provided. Given the lack of consensus on language preferences, this paper uses both identity-first and person-first language (e.g. Kenny et al., 2016).
Influence of COVID-19 on autistic individuals and their families
Families of autistic children may have been particularly vulnerable to pandemic-related disruptions due to the core characteristics of ASD. ASD is a neurodevelopmental disorder characterized by early-onset difficulties in social communication, social-emotional reciprocity, hyper- and/or hyposensitivity to sensory inputs and restricted and repetitive behaviors (APA, 2022). ASD is also associated with high rates of co-occurring anxiety, depression, behavioral/conduct problems and attention-deficit/hyperactivity disorder (see review Lai et al., 2019). The COVID-19 pandemic provided an opportunity to examine how sudden changes in daily life influenced autistic children’s development and parenting stress.
Autism symptoms
Autistic children, who often prefer routine and consistency, faced added challenges due to the pandemic’s unpredictability (Smile, 2020). Studies conducted during the pandemic found increased autistic traits, repetitive behaviors, and reduced access to effective therapy (Asbury and Toseeb, 2023; Colizzi et al., 2020; Levante et al., 2021; Renzo et al., 2020; White et al., 2021). In addition, reduced access to clinical care may have influenced how autistic youth manage daily changes, potentially exacerbating autism-related symptoms and behaviors (Renzo et al., 2020). However, autistic children and adults reported relief from reduced social pressure, social distancing measures and adapted socialization that came with the added COVID-19 safety measures (Bellomo et al., 2020; Castelein et al., 2021).
Emotional and behavioral functioning
Findings on emotional and behavioral functioning throughout the pandemic varied (see review: Ahmed et al., 2022). Some studies showed that compared to a pre-pandemic period, autistic youth were found to have poorer overall mental health (Turner et al., 2023), increased aggression, hyperactivity, anxiety, depression, fear and restricted and repetitive behaviors (Martínez-González et al., 2021) and greater emotional symptoms (Amorim et al., 2020; Nonweiler et al., 2020). These challenges extended into adulthood with autistic adults reporting poor mental health (Davidson et al., 2021; Riese and Mukherjee, 2022) and increased rigidity during the pandemic (Riese and Mukherjee, 2022). However, other studies found that autistic children appeared happier and calmer during the COVID-19 period (Mumbardó-Adam et al., 2021), potentially due to reduced social stressors and changes in school environments (Clark and Adams, 2020). These mixed findings highlight the need to better understand the impact of the pandemic conditions on autistic symptoms and emotional and behavioral functioning relative to normative development.
Parenting stress
Within children’s social environment, parents play a paramount role in their development (Smith et al., 2014; Zaidman-Zait et al., 2014), but for parents of autistic children, this role often comes with different challenges (Schieve et al., 2007). During “typical” periods, parents of autistic children report greater parenting stress compared to non-ASD groups (Padden and James, 2017). Parenting stress refers to the negative feeling prompted by a misalignment between the demands of parenting and resources of support (Abidin, 1995; Padden and James, 2017). During the COVID-19 pandemic, this stress was further amplified by disruptions in education, socialization and therapy (Amirova et al., 2022; Dhiman et al., 2020; Mazzoni et al., 2022). Some parents of autistic children reported higher levels of anxiety and stress, disrupted routines and isolation (Ameis et al., 2020; Colizzi et al., 2020; Dhiman et al., 2020; Ersoy et al., 2020; Haidar and Meadan, 2024; Manning et al., 2021; Ueda et al., 2021). Conversely, others found relief from reduced social and societal pressures and reduced worry regarding their autistic child (Ameis et al., 2020). Some parents reported learning more about their child and benefiting from exploring new strategies to involve their child in family routines, a potential advantage of parents spending more time at home with their children (Mumbardó-Adam et al., 2021; Tokatly Latzer et al., 2021). As parenting stress is associated with adjustments in biological and psychological factors in both the parent and child’s life, there is a need to better understand parenting stress during crises (Dijkstra-de Neijs et al., 2020). Understanding how parents respond to stress can inform targeted supports such as problem-solving strategies, resources for self-care and policy-level initiatives.
Current study
The COVID-19 pandemic presented an opportunity to examine how major life events and stressors affect families of autistic children. This study aimed to compare autistic children’s social differences and their emotional and behavioral functioning along with parenting stress during a pandemic and nonpandemic period. Given the relative stability of autism traits (Louwerse et al., 2015), we hypothesized no significant differences in social symptom development across cohorts. However, we hypothesized greater increases in emotional and behavioral challenges in children and adolescents exposed to COVID-19 safety measures compared to those in a typical developmental context (e.g. Ahmed et al., 2022; Amorim et al., 2020; Mutluer et al., 2020; Nonweiler et al., 2020; Renzo et al., 2020). As previous literature described both feelings of increased stress and relief during the pandemic, we aimed to explore how parenting stress varied across the domains of parent–child relationship problems, parenting problems, depressive mood, parental role restriction and physical health problems between parents during the COVID-19 pandemic and parents 10 years before the COVID-19 pandemic (e.g. Alhuzimi, 2021; Amorim et al., 2020; Colizzi et al., 2020; Dhiman et al., 2020; Gillespie-Smith et al., 2021).
Method
Procedures
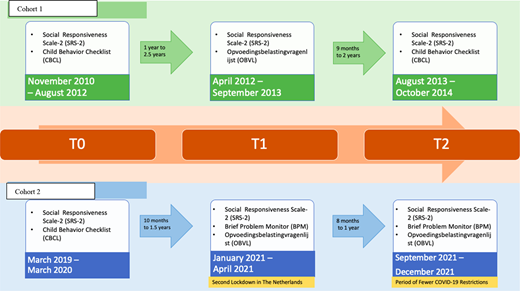
Data from two cohorts, Cohort 1 (Social Spectrum Cohort: Duvekot et al., 2017) and Cohort 2 (Rotterdam Autism Consortium: Dekker et al., 2022), comprised children and adolescents with a clinical diagnosis of ASD and their families from one of the three prominent mental health-care institutions in the Rotterdam region of the Netherlands. Data were collected at three time points (T0, T1 and T2) with approximately similar intervals between time points. A visual representation of the cohorts, timeline and measurements is provided (Figure 1). Data in Cohort 1 were collected 6–10 years before the COVID-19 pandemic. In Cohort 2, the COVID-19 pandemic began after T0. This led to significant adaptations in everyday life, such as the closing of schools, working from home (children and parents), quarantines, social distancing and mask mandates at T1 and T2; however, by T2 COVID-19 restrictions were less severe, namely, fewer social distancing requirements and increased COVID-19 testing [National Institute for Public Health and the Environment of The Netherlands (RIVM), 2022]. Cohort 1 recruited participants ages 2½ to 10, while Cohort 2 recruited participants ages 4 to 21. Given the age difference between cohorts, age was controlled for where relevant. Table 1 shows the participant demographic information. Parents consented to data collection from their clinical file (T0) and completed online questionnaires about themselves and their autistic child at T1 and T2. Participants in Cohort 1 received compensation for their travel expenses and children were offered a small prize and participants in Cohort 2 received graded compensation of €10 at T1 and €25 at T2 to help promote long-term participation and minimize dropout. Local medical ethics committees approved both the Blinded and Blinded studies (ethical approvals blinded for review).
Measures and participants
Measures and participants were organized by theme. Power calculations were conducted separately for each theme, providing estimates for the ability to detect small and medium effect sizes. Detecting smaller effects typically requires larger sample sizes, as such effects are more susceptible to being obscured by measurement error or variability (Cohen, 2013).
Autism symptoms.
The Social Responsiveness Scale-2 (SRS-2), school-age version for children 4–18, measured autistic traits at T0, T1 and T2 (Constantino, 2013). The 65-item parent-report questionnaire used a four-point Likert scale (“not true” to “always true”). Both total scores (ranging from 0 to 195, with higher scores indicating more severe deficits in social interactions) and clinical subdomain scores on “awareness” (eight items), “cognition” (12 items), “communication” (22 items), “motivation” (11 items) and “restricted and repetitive behaviors” (12 items) were analyzed. The SRS-2 has strong reliability and validity (Bruni, 2014). Cohort 1 inclusion criteria required a total raw score of 75 or higher aligning with Constantino (2013) guidelines for ASD (Duvekot et al., 2017). This criterion was not applied to Cohort 2, as all participants had a clinical autism diagnosis (Dekker et al., 2022). To evaluate whether the two cohorts were comparable in terms of autism severity at baseline, an independent samples t-test was conducted on the SRS-2 total and subscale scores. Results revealed no significant differences between the groups at T0: total score t(88) = 0.22, p = 0.83, Social Awareness t(88) = −0.23, p = 0.82, Social Cognition t(88) = 0.58, p = 0.56, Social Communication t(88) = −0.12, p = 0.45, Social Motivation t(88) = −1.53, p = 0.07, Restricted and Repetitive Behaviors t(88) = 0.96, p = 0.17. These findings suggest that the cohorts did not differ significantly in autism severity at the initial assessment.
To allow for direct comparison, participants were only included if they were four years or older at T0, resulting in 92 participants (Cohort 1: n = 66, Cohort 2: n = 26). Power analysis indicated that n = 92 provided 99% power to detect a medium effect size (d = 0.5) and 53% power for a small effect size (d = 0.2) in a repeated-measures analysis of variance (ANOVA) with two groups, three-time measurements and five measurements for the SRS-2 subscales (Faul et al., 2009).
Emotional and behavioral functioning
The Brief Problem Monitor (BPM) assessed emotional and behavioral functioning at T0 and T2 (Achenbach et al., 2011). This 19-item parent-report questionnaire, derived from the Child Behavior Checklist (CBCL) (Achenbach and Rescorla, 2001), uses a three-point Likert scale from “not at all” (0) to “very true” (2). The BPM total score, ranging from 0 to 30, and three subscales Internalizing (six items), Externalizing (seven items) and Attention (six items), were analyzed. Higher scores indicate more problems in children. The BPM has good reliability and validity (Piper et al., 2014).
Participants who originally completed the CBCL had their scores converted to BPM equivalents so that all analyzed data was scored based on the BPM. To ensure uniform BPM/CBCL use, participants younger than five were excluded to ensure consistent use of CBCL cut-offs of 6–18. The final sample included 61 participants (Cohort 1: n = 37, Cohort 2: n = 24). Power analysis indicated that n = 61 provided 97% power to detect a medium effect size (d = 0.5) and 34% power for a small effect size (d = 0.2) in the group * time interaction for using a repeated measure ANOVA with two groups and two-time measurements and three measurements for the BPM subscales (Faul et al., 2009).
Parenting stress
The Parenting Stress Questionnaire [Opvoedingsbelastingvragenlijst (OBVL) in Dutch; Vermulst et al., 2015] assessed parenting stress at T1. The 34-item parent-report questionnaire uses a four-point Likert scale (“not true” to “very true”). Total scores range from 34 to 136, with lower scores indicating lower levels of parenting stress. The subdomains include parent–child relationship problem with six items measuring the degree to which the parent views their relationship with their child as stressful, parenting problems domain with seven items referring to the degree to which the parent perceives raising the child as stress inducing, depressive mood domain with seven items measuring the degree in which a parent is unhappy with themselves or their living conditions, parental role restriction domain with six items referring to how much the parent feels restricted in one’s freedom and their frustrations with trying to maintain their own identity and physical health problems domain with eight items relating to the degree in which the parent feels physically healthy and fit. Whereas the total score provides a broad index of parenting stress, examination of subscales allows for examination of differential patterns in parenting that may be potentially masked when relying on a global stress score. The Dutch OBVL shows good reliability and validity (Vermulst et al., 2015), even during periods when increased stress is expected, such as when a child is sick (Conijn et al., 2022).
The final sample included 115 participants (Cohort 1: n = 66, Cohort 2: n = 49), providing 99% power to detect a medium effect size (d = 0.5) and 77% power for a small effect size (d = 0.2) in the group * subscale interaction using a repeated measure ANOVA with two groups and five measurements for the OBVL subscales (Faul et al., 2009).
Analyses
The data were coded and cleaned according to the manuals of their respective questionnaires. Analyses were determined by research aim. Null hypothesis tests were conducted using IBM SPSS version 29, and Bayesian analyses were conducted using JASP version 0.143.
Autism symptoms
Repeated-measures ANOVA with Greenhouse–Geisser corrections assessed social trait development with SRS-2 total and subscale scores as the dependent variable, cohort group (Cohort 1 vs Cohort 2) as a between-subject factor, the three-time points (T0, T1 and T2) and SRS-2 subscale (Social Awareness, Social Cognition, Social Communication and Restricted and Repetitive Behaviors) as within-subjects factors. Two outliers were excluded due to absolute standardized residual scores greater than 3 and having influence on the sample, resulting in n = 90 (Cohort 1: n = 66, Cohort 2: n = 24). Given the difference between ages in the two samples and its known relationship to autism symptoms, analysis included age as a covariate (Gotham et al., 2012).
Emotional behavioral functioning
Repeated-measures ANOVA with Greenhouse–Geisser corrections explored emotional and behavioral functioning with BPM subscale score as the dependent variable, cohort group (Cohort 1 vs Cohort 2) as a between-subject factor, the two time points (T0 vs T2) and BPM subscale (Internalizing, Externalizing and Attention) as within-subjects factors. Analyses were run again including age as a covariate. No outliers were identified.
Parenting stress
Repeated-measures ANOVA with Greenhouse–Geisser corrections examined parenting stress at T1 with OBVL subscale score as the dependent variable, cohort group (Cohort 1 vs Cohort 2) as between-subject factor, and OBVL subscale (Parent–child Relationship Problems, Parenting Problems, Depressive Mood, Parental Role Restrictions and Physical Health Problems). Before data analysis, three outliers were identified due to having an absolute standardized residual score greater than 3; however, when checking their influence, only two outliers greatly impacted the slope of the regression line and therefore were removed (Andrews and Pregibon, 1978). As a result, we used a sample size of 113 participants, with 64 participants in Cohort 1 and 49 in Cohort 2. Analyses were run again including age as a covariate.
Results
Descriptive statistics of each cohort by research aim can be found in Table 2.
Autism symptoms
Greenhouse–Geisser corrections were applied to all within-subjects effects in the repeated-measures ANOVA. Both the main effect of group, F(1, 87) = 0.32, p = 0.57, ηp2 = 0.004 and the group * time interaction, F(1.88, 163.53) = 0.76, p = 0.46, ηp2 = 0.009, were not significant, suggesting the cohorts showed similar levels and temporal development of the children’s autism symptoms (Table 3). The same pattern of results was found when excluding age as a covariate. No post hoc analyses were conducted, as no significant omnibus effects were observed. To further investigate whether the data could provide evidence against this group * time interaction effect, a JZS Bayes factor repeated-measures ANOVA with default prior scales, which included the same factors and covariate, was performed (Rouder et al., 2012). The Bayes factor (BF = 20.02) indicated strong evidence in favor of the null model over the alternative that included the group × time interaction. This means the data were 20 times more likely to occur under the model without the interaction, providing strong evidence that the two cohorts did not differ in their developmental of autism symptoms (for more details on the Bayes factor classification scheme see Van Doorn et al., 2021).
Emotional and behavioral functioning
Greenhouse–Geisser corrections were applied to all within-subjects effects with more than two levels in the repeated-measures ANOVA. Both the main effect of group, F(1, 57) = 0.24, p = 0.24, ηp2 = 0.004 and the group * time interaction, F(1, 57) = 1.07, p = 0.31, ηp2 = 0.018, were not significant, suggesting that the cohorts showed similar levels and temporal development of emotional and behavioral functioning, while correcting for potential age differences (Table 4). No post hoc corrections were applied. The same pattern of results was found when excluding age as a covariate. Similar JZS Bayes factor repeated-measures ANOVA with default prior scales was performed (Rouder et al., 2012). Across all models, models excluding the group * time interaction were preferred to models that included it by a Bayes factor of 12.78. This provides strong evidence against the hypothesis that the two cohorts differed in their development of emotional and behavioral functioning, suggesting that these outcomes remained consistent across cohorts.
Parenting stress
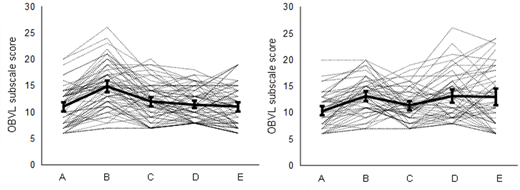
Greenhouse–Geisser corrections were applied to the within-subjects effect in the repeated-measures ANOVA was performed. An expected main effect of OBVL subscale, F(2.66, 292.42) = 4.84, p < 0.01, ηp2 = 0.042 was found (Table 5). A nonsignificant main effect of group, F(1, 110) = 0.84, p = 0.36, ηp2 = 0.008, but a significant group * subscale interaction, F(2.66, 292.42) = 10.64, p < 0.001, ηp2 = 0.088 (Figure 2) was found, suggesting the cohorts showed similar levels, but different profiles of parenting stress at T1, while correcting for potential age differences. The same pattern of results was found when excluding age as a covariate. Follow-up contrasts indicated that Cohort 2 showed significantly lower levels of Parenting Problems, t(111) = 2.17, p = 0.03, but significantly higher levels of Parental Role Restrictions t(111) = 2.54, p = 0.01 and Physical Health Problems t(111) = 2.24, p = 0.03. To investigate whether the data could provide evidence for this group * time interaction, a JZS Bayes factor repeated-measures ANOVA with default prior scales which included the same factors and covariate was performed (Rouder et al., 2012). Across all models, models including the group * subscale interaction were preferred to models that excluded it by a BF of 2,728, providing very strong evidence for the hypothesis that the two cohorts differed in their profiles of parenting stress at T1.
Discussion
The COVID-19 pandemic altered daily life, requiring children and their parents to adapt to new social rules, quarantines and public safety measures. This study provides exploratory comparisons, due to the wide age range and cohort differences, that may aid in considering the influence of stressors, such as global pandemics, on families of autistic children. Findings suggest that while autistic children’s developmental trajectories are similar 10 years before the pandemic to during the pandemic, parents during the pandemic experienced fewer parenting problems, but more role restriction and physical health problems than their prepandemic peers.
Impact on child development
The developmental trajectory of social symptoms and emotional and behavioral functioning did not differ significantly between cohorts. As hypothesized, social symptoms remained stable over time, consistent with the stability of the diagnosis. Contrary to expectations, parents did not report increased challenges in emotional and behavioral functioning in their autistic children during the pandemic compared to typical maturation.
Most prior studies lacked pre-pandemic comparison data, making it difficult to attribute findings to the influence of the COVID-19 safety measures (e.g. Amorim et al., 2020; Colizzi et al., 2020; Gotham et al., 2012; Levante et al., 2021; Renzo et al., 2020). Our findings align with research suggesting that observed symptoms during the pandemic may reflect ongoing challenges. A study that compared emotional and behavioral problems during the COVID-19 pandemic to a prepandemic period similarly found that autistic participants’ changes in emotional and behavioral problems remained relatively stable between the two periods (de Maat et al., 2022). Together, these results indicate that parent-reported symptoms were comparable across time, reinforcing the need to identify resilience factors that help autistic children adapt during disruptions such as the COVID-19 pandemic.
Impact on parenting stress
Parents during the COVID-19 pandemic reported fewer parenting problems, but greater role restriction and physical health problems compared to those in a non-pandemic period. The shift toward hybrid or remote working may have contributed to greater work–life balance and increased flexibility with work. In addition, reduced social pressures (Ameis et al., 2020) and greater time at home may have alleviated some parenting challenges by fostering greater understanding and connection with their children as previously reported in other studies (Mumbardó-Adam et al., 2021; Tokatly Latzer et al., 2021). However, parents were also required to fill additional roles of educators and therapists to support their children during the pandemic (Dhiman et al., 2020) whilst external support was reduced or completely stopped. This means there was not only added parenting responsibilities but also a reduction of breaks in caregiving that came from their child working with educators or therapists. Qualitative reports mimic these findings (van Rijen et al., 2025). However, it is possible that increased physical health problems reflect general somatic distress linked the health consequences of COVID-19 rather than stress resulting from parenting demands. Similarly, parental role restrictions may stem from competing demands, such as the expectation to maintain work responsibilities while providing full-time caregiving, reflecting broader role restrictions rather than child specific.
Although both cohorts were drawn from the same institutions, differences in reported parenting stress may reflect more than just the direct impact of the COVID-19 pandemic. Evolving diagnostic practices, shifting societal expectations or changes in service provision may also have contributed. Moreover, increased parenting stress during the pandemic may not solely reflect difficulties related to the child, but rather the broader strain of navigating competing roles, such as being expected to maintain full-time work while providing full-time caregiving. In this context, parental role restrictions may partly stem from external demands (e.g. public health mandates, employer expectations) rather than increased child needs. Notably, while children’s functioning appeared relatively stable, parenting experiences varied. Specifically, some parents reported relief from reduced external obligations, while others faced heightened burdens. These findings underscore the importance of targeted family supports, such as respite care, remote interventions and self-care programs, particularly during times of societal disruption when the boundary between caregiving and other responsibilities becomes increasingly blurred.
Limitations
This study compared two cohorts of autistic children and their families at distinct time points, one during a global pandemic and one during a nonpandemic period. Although both cohorts were drawn from the same region and service providers, the temporal gap between data collection of the cohorts may reflect differences in diagnostic practices, services and supports available as well as other societal changes. In addition, some PSQ subscales (e.g. physical health, role restriction) may reflect broader pandemic-related stress rather than parenting stress specifically. Furthermore, as this study was developed in response to the unexpected COVID-19 pandemic, cohorts were not perfectly matched. Cohort 1 (Duvekot et al., 2017) had a larger sample size than cohort 2 (Dekker et al., 2022), and both were relatively small. Cohort 1 included children between the ages of 2.5–10 years old, while Cohort 2 included individuals between the ages of 4 and 21 years old. Whereas age was controlled for as a covariate, future research may compare age by groups such as school or developmental level. Both cohorts had more biological male than female participants, a common trend in autism research due to autism being more commonly diagnosed in males and underdiagnosed in females (Halladay et al., 2015). Further exploration is important to ensure that autism research is understood in both males and females. Despite these limitations, this study offers a rare opportunity to examine parenting stress and autistic child development during a prolonged period of societal disruption compared to a period in which such global disruption was not present. Future studies should consider longitudinal designs with matched samples to isolate pandemic-specific effects more precisely.
Conclusion
Within this study, parents were not reporting unique development of their child’s autism symptoms or emotional and behavioral functioning during the pandemic compared to a nonpandemic period. However, parents reported more parental role restriction and physical health problems despite fewer parenting problems during the pandemic. These findings highlight the need to support parents, as stressors affecting parents can create a ripple effect throughout the family. While the pandemic introduced many challenges, it also appeared to positively impact some areas of parenting stress, such as reduced societal and work pressures, enabling parents to spend more structured time with their children. Many parents reported engaging in schoolwork and goal-oriented activities with their children, leading to the development of new strategies for support, such as fostering strengths-based activities and creating structured home routines (Tokatly Latzer et al., 2021). The tools and coping mechanisms learned during the pandemic may prove useful in future times of stress or disruption. Overall, the pandemic has led to a greater acknowledgment that parents, especially, those of children with disabilities, need added support, such as respite services, remote interventions and self-care programming, during periods of stress/challenge which in turn will allow parents to be better equipped to support their children.
The authors graciously acknowledge all of the participants in this study without whom this research would not be possible.
Funding
The Social Spectrum Study cohort is supported by a grant from the Sophia Foundation for Scientific Research (SSWO Project Number 958). The Research Autism Consortium cohort ASD & COVID-19 stu d y is supported by a grant from the Netherlands Organization for Health Research and Development (ZonMw), within the program ‘COVID-19 Focus area 2. Care and prevention, Theme 2: Care and prevention for vulnerable citizens’ (project number: 10430022010007). Olivia F. Ward gratefully acknowledges financial support for her time by the Fulbright U.S. Student Program, which is sponsored by the U.S. Department of State and the Netherlands-America Foundation. The contents of the manuscript are solely the responsibility of the author and do not necessarily represent the official views of the Fulbright Program, the Government of the United States, or the Netherlands-America Foundation.