Hospital buildings are highly energy-intensive, with HVAC systems critical to reliability, energy use and indoor environmental quality. Despite the potential of predictive maintenance (PdM), its adoption in hospital facilities management remains limited. This study aims to develop an IoT-enabled PdM framework to support HVAC maintenance decision-making while aligning maintenance practice with sustainability objectives.
An explanatory sequential mixed-methods design was adopted, comprising a survey of hospital HVAC maintenance practices and digital readiness, followed by expert interviews to contextualise feasibility, workflow integration and organisational constraints. Findings from both phases informed development of a layered PdM framework.
Results reveal uneven organisational readiness, marked by high HVAC criticality but limited digital infrastructure, skills and data integration. Preventive maintenance remains dominant, although PdM is viewed favourably when compatible with existing workflows. These drivers informed a phased, system-agnostic framework integrating sensing, analytics, decision-support and performance feedback.
The framework provides a structured pathway for phased PdM adoption, supporting improved maintenance planning, HVAC reliability and alignment between maintenance practice and sustainability goals.
This study contributes an empirically grounded PdM framework that links HVAC maintenance decision-making with energy performance and sustainability outcomes, bridging technical PdM research and facilities management practice in hospital environments.
1. Introduction
1.1 Energy, operational and maintenance challenges in hospital buildings
Hospital buildings are among the most energy-intensive facility types due to continuous operation, stringent indoor environmental requirements and high ventilation and cooling demands (Balaras et al., 2007; Čongradac et al., 2012). Across both advanced and emerging economies, HVAC systems account for a substantial share of hospital energy consumption, making them critical to operational efficiency, climate resilience and continuity of healthcare services (García-Sanz-Calcedo et al., 2019; Teke and Timur, 2014). Rising global temperatures and increasing heatwave frequency are further intensifying cooling demand, increasing operational costs and placing additional stress on mechanical systems (Perkins-Kirkpatrick and Lewis, 2020). At the same time, ageing HVAC assets and suboptimal maintenance practices contribute to avoidable energy waste, premature equipment failure and disruptions to clinical operations (Katipamula and Brambley, 2005).
In response to energy security and decarbonisation pressures, hospitals have increasingly adopted on-site renewable energy solutions, particularly solar photovoltaic systems (IEA, 2022; WHO, 2023). However, the effectiveness of such investments is strongly conditioned by the operational efficiency of end-use equipment, especially HVAC systems, which remain the largest electricity consumers in hospitals (Teke and Timur, 2014). Poorly maintained HVAC assets can offset renewable energy gains by increasing baseline demand and accelerating system degradation. This underscores the need to view renewable energy deployment and PdM as complementary strategies, where effective maintenance is essential for translating low-carbon energy supply into sustained operational performance.
Despite this, hospital HVAC maintenance remains dominated by corrective and time-based preventive approaches, with interventions typically triggered by equipment failure, occupant complaints or fixed service schedules rather than by real-time system condition (Alghanmi et al., 2022; Lavy and Shohet, 2004). These practices provide limited visibility of early-stage faults and allow inefficiencies to persist between inspections, resulting in unplanned downtime and excessive energy consumption (Pérez-Lombard et al., 2008). In many healthcare settings, particularly those with constrained resources, maintenance decisions are further shaped by budget limitations, fragmented documentation and reliance on tacit technician experience rather than data-driven diagnostics.
Although digital building technologies have advanced significantly, PdM remains unevenly adopted in healthcare facilities (Li et al., 2023). In high-income contexts, interoperability challenges, equipment heterogeneity and cybersecurity concerns limit the integration of advanced predictive solutions (Argaw et al., 2020; Kelly et al., 2020). In middle- and low-income settings, additional barriers include limited instrumentation, ageing infrastructure and insufficient technical capacity (Adair-Rohani et al., 2013). Across contexts, the continued reliance on reactive maintenance undermines both energy efficiency and HVAC reliability. Given the critical role of HVAC systems in infection control, patient safety and clinical functionality, these limitations point to a global need for maintenance models that use real-time data to anticipate failures and optimise performance proactively (Memarzadeh and Xu, 2012).
1.2 Limitations of existing maintenance and sustainability assessment approaches
IoT-enabled PdM has demonstrated strong potential to improve HVAC performance through continuous monitoring, anomaly detection and prognostics (Tian et al., 2023; Zonta et al., 2020). Evidence from commercial and industrial buildings indicates that PdM can reduce HVAC energy consumption, decrease downtime and extend equipment lifespan (Aghili et al., 2024; Bousdekis et al., 2020). Despite these benefits, empirical implementation of PdM in hospital environments remains limited.
Adoption is constrained by challenges related to legacy system integration, insufficient sensor coverage, low digital maturity, high initial investment costs, limited data analytics expertise and organisational resistance to AI-enabled decision-support systems (Bokrantz et al., 2020; Li et al., 2023; Psomas et al., 2021). Additional concerns regarding system complexity, data governance and long-term maintenance of digital infrastructure further inhibit uptake, particularly in resource-constrained healthcare settings (Amiri et al., 2021). These barriers highlight the need for PdM architectures that align technological capabilities with hospital workflows, energy management priorities and sustainability objectives.
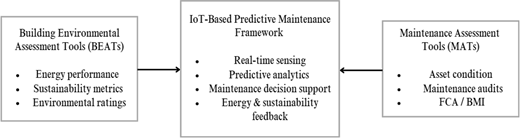
Existing assessment tools provide limited support for such integration. Building Environmental Assessment Tools (BEATs) focus on benchmarking environmental performance and management policies but offer little insight into asset-level maintenance practices or real-time system degradation, particularly for HVAC systems (Berardi, 2012; Ding, 2008; Haapio and Viitaniemi, 2008) On the other hand, Maintenance Assessment Tools (MATs) emphasise asset condition and maintenance planning but rely largely on periodic inspections and static records, with weak linkage to energy performance and sustainability outcomes (Dejaco et al., 2017; Harvey et al., 2017; Re Cecconi et al., 2019). As a result, sustainability assessment and maintenance practice remain largely disconnected, limiting the capacity of existing tools to support data-driven PdM in hospital environments. Figure 1 illustrates the disconnect between existing sustainability assessment tools and maintenance assessment approaches, highlighting the need for an integrated IoT-enabled PdM framework.
1.3 Aim and contributions of the study
This study aims to develop an IoT-enabled PdM framework for hospital HVAC systems that enhances energy efficiency, operational resilience and sustainability in resource-constrained environments. Operational resilience is defined here as the capacity of HVAC systems to maintain reliable environmental control and service continuity under conditions of equipment degradation, maintenance constraints and external stressors such as extreme heat events or energy supply disruptions.
The study makes four main contributions. Firstly, it proposes a multi-layered PdM framework tailored to the operational and organisational realities of hospital HVAC systems. Secondly, it synthesises insights from maintenance management, digitalisation, sustainability and HVAC performance literature. Thirdly, it integrates perspectives from BEATs and MATs to bridge the gap between environmental assessment and PdM. Finally, it presents a context-sensitive framework validated through empirical evidence and expert input, designed to be adaptable across both advanced and emerging healthcare systems. Although empirically informed by hospitals in Nigeria, the framework is intended to be transferable to healthcare facilities operating under similar organisational and resource constraints globally.
2. Literature review
Maintenance practices in buildings have evolved from reactive and calendar-based routines towards more data-enabled approaches, driven by advances in sensing, connectivity and cyber-physical integration. While preventive maintenance is more structured than corrective maintenance, it can be inefficient because schedule-driven interventions often do not reflect actual equipment condition and may allow degradation to accumulate between inspections (Jardine et al., 2006). Condition-based maintenance improves responsiveness, but reliance on manual checks and intermittent measurements can still limit fault visibility and slow decision-making (Jardine et al., 2006). PdM addresses these limitations through continuous monitoring and analytics that detect anomalies and anticipate degradation before failure occurs (Zonta et al., 2020).
The growth of the Internet of Things (IoT) has accelerated PdM adoption across the built environment by enabling distributed sensing at relatively low cost. Typical IoT architectures integrate sensors, microcontrollers, gateways and communication protocols that transmit operational data to cloud platforms for storage, analysis and decision support (Lee and Lee, 2015; Perera et al., 2014). Such configurations support continuous monitoring of building systems including HVAC components, pumps, fans and electrical subsystems using indicators such as temperature, vibration, power signatures, humidity and flow (Jia et al., 2019). Machine-learning techniques such as anomaly detection, clustering and remaining useful life estimation are increasingly combined with building-domain rules and expert knowledge to improve diagnostic reliability under variable loads and operating conditions (Dalzochio et al., 2020; Lei et al., 2018).
However, PdM implementation in buildings remains challenging. Many IoT-enabled PdM initiatives focus on algorithmic accuracy while giving less attention to practical integration requirements such as sensor placement, data governance, workflow redesign and interoperability between legacy building management systems (BMS) and newer IoT platforms (Fina et al., 2019; Psomas et al., 2021). Industrial sectors have advanced further by embedding PdM within structured asset-management systems and digital-twin platforms, yet these templates do not transfer neatly to buildings due to differences in occupancy patterns, regulatory constraints and comfort requirements (Bokrantz et al., 2020).
In healthcare facilities, the stakes are higher because HVAC performance is tightly linked to infection control, patient comfort, and continuity of clinical services. Yet the evidence base remains fragmented: computer science research often prioritises modelling and sensing performance, while facilities-management studies emphasise governance, resourcing and operational constraints (Lavy and Shohet, 2004). As a result, there is limited guidance on how sensing, analytics, human expertise and organisational processes should be configured as an integrated PdM system within hospital environments.
Because HVAC systems account for a substantial share of hospital energy use and influence clinical operations, they are central to PdM research. Early foundational work focused on rule-based and physics-based fault detection and diagnosis (FDD), using expert rules or models to identify abnormal behaviour in coils, compressors, valves and sensors (Katipamula and Brambley, 2005). With increased availability of high-resolution building data, data-driven methods such as neural networks, support vector machines and ensemble classifiers have demonstrated strong performance for detecting HVAC faults across diverse operating conditions (Aghili et al., 2024; Amasyali and El-Gohary, 2018). Hybrid approaches that combine model-based reasoning with machine-learning outputs can improve robustness under dynamic load profiles and occupancy variation (Zhuang et al., 2023).
Beyond diagnostics, predictive and optimisation-based control approaches have been linked to improved HVAC energy efficiency. Model predictive control, reinforcement learning and adaptive methods can proactively schedule equipment operation to reduce energy use while maintaining strict comfort and air-quality constraints (Afram and Janabi-Sharifi, 2014; Oldewurtel et al., 2012). Digital-twin approaches extend these capabilities by maintaining real-time virtual representations of HVAC assets, enabling simulation of degradation, performance forecasting and maintenance scenario analysis Boje et al. (2020); Sacks et al. (2020).
Hospitals differ materially from many commercial buildings because they require precise control of temperature, humidity and airflow across diverse clinical zones, including operating theatres, isolation wards, laboratories and intensive care units (Beggs et al., 2008; Čongradac et al., 2012; Memarzadeh and Xu, 2012). These requirements heighten the risks associated with undetected faults, which may compromise air-cleanliness standards, patient safety and clinical equipment performance. Inadequate HVAC maintenance has also been linked to outbreaks of airborne and waterborne pathogens, reinforcing the public-health implications of system degradation (Llewellyn et al., 2017; Yao et al., 2024). In addition, the literature often assumes highly instrumented central HVAC infrastructure, even though many hospitals particularly in Asia, Africa and parts of Europe operate decentralised split-unit or packaged systems with limited BMS integration (Teke and Timur, 2014). Consequently, many hospital PdM studies remain limited to isolated algorithms or small-scale pilots, offering limited guidance on organisational coordination and workflow integration.
The maintenance–energy–sustainability link is increasingly recognised as a critical but underdeveloped dimension of building performance. While energy-efficiency strategies often emphasise design optimisation, controls and retrofit technologies, inadequate maintenance can erode expected gains by driving systems away from optimal performance (Alghanmi et al., 2022). Component degradation including fouled heat exchangers, refrigerant leakage, sensor drift and worn fans can lead to persistent energy waste even in buildings with advanced controls (Katipamula and Brambley, 2005). In hospitals, where continuous operation and strict indoor environmental requirements create high baseline demand and low tolerance for downtime, maintenance failures increase both energy consumption and operational risk (Memarzadeh and Xu, 2012). Poor maintenance can also trigger premature replacement and higher material waste, increasing embodied impacts across the lifecycle (Sartori et al., 2012). PdM offers a pathway to mitigate these outcomes by supporting earlier detection of degradation and targeted intervention before inefficiencies become systemic (Es-sakali et al., 2022; Zonta et al., 2020). However, achieving these benefits requires integrated approaches that connect maintenance decision-making with energy performance objectives, operational risk management and sustainability assessment, rather than treating these domains separately (Bousdekis et al., 2020).
This separation is evident in existing assessment tools. BEATs such as BREEAM, LEED, Green Star, CASBEE and SBTool benchmark environmental performance across energy, indoor environmental quality, materials and emissions (Berardi, 2012; Cole, 2005; Ding, 2008; Haapio and Viitaniemi, 2008). However, they primarily assess performance outcomes or management policies and provide limited insight into asset-level maintenance practices or real-time degradation processes; maintenance is rarely treated as an active mechanism for sustaining performance (Doan et al., 2017; Scofield, 2013). Conversely, MATs, including Facility Condition Assessments, Building Maintenance Indices, maintenance audits and reliability-centred maintenance frameworks, focus on asset condition and prioritisation but rely largely on periodic inspections, historical records and expert judgement rather than continuous operational data (Edirisinghe et al., 2013; Harvey et al., 2017; Re Cecconi et al., 2019). MATs also tend to operate independently of energy and sustainability evaluation, limiting their usefulness for linking maintenance actions to environmental outcomes (Alghanmi et al., 2022).
As a result, BEATs and MATs offer complementary but disconnected perspectives: BEATs prioritise sustainability outcomes without engaging with maintenance mechanisms, while MATs address condition and planning without explicitly linking decisions to energy and sustainability performance. This disconnect is particularly problematic in hospital settings, where HVAC systems are mission-critical and PdM requires continuous sensing, real-time analytics, risk-based prioritisation, and coordination across technical and clinical domains (Psomas et al., 2021; Zonta et al., 2020). Table 1 compares the strengths and limitations of BEATs, MATs, and the proposed IoT-enabled PdM approach.
3. Methodology
3.1 Research design
This study adopts a mixed-method explanatory sequential research design within a pragmatic research paradigm. This approach combines an initial quantitative phase with a subsequent qualitative phase, allowing quantitative findings to be explained and contextualised through expert insight before being synthesised into a PdM framework. The design is well suited to practice-oriented research where both system-level patterns and contextual realities must be addressed to inform actionable solutions.
In Phase 1, a structured survey was used to examine prevailing HVAC maintenance practices, levels of digital readiness and perceptions of IoT-enabled PdM within hospital facilities. The quantitative phase provided a broad empirical overview of dominant trends, constraints and priorities relevant to maintenance decision-making and digital transformation. In Phase 2, semi-structured expert interviews were conducted to interpret and elaborate on the survey findings, with particular emphasis on implementation feasibility, system integration challenges and organisational constraints that could not be fully captured through survey data alone. In the final stage, insights from both data strands were synthesised to inform the design of an IoT-enabled PdM framework tailored to hospital HVAC systems.
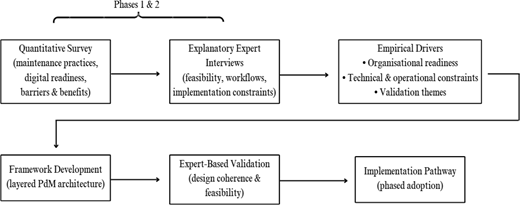
Rather than treating quantitative and qualitative findings as parallel outputs, the study integrates them sequentially, with each phase informing the next. The explanatory sequential research design and its role in guiding framework development are illustrated in Figure 2, where empirical drivers represent inputs derived from the data-generation phases rather than components of the research design itself.
3.2 Quantitative survey and explanatory expert interviews
The empirical component followed a two-phase explanatory sequential structure, comprising a quantitative survey followed by qualitative expert interviews. The survey captured current HVAC maintenance practices, levels of digitalisation and perceptions of IoT-based PdM among hospital facility managers, HVAC engineers, maintenance supervisors and technical personnel involved in building services operation. Respondents were selected based on their direct involvement in maintenance planning, execution and system oversight.
Survey items addressed maintenance strategies, documentation practices, perceived benefits and barriers associated with PdM, and organisational conditions influencing maintenance decision-making. Data were analysed using descriptive statistics and selected inferential techniques to identify patterns with direct relevance to framework design, rather than to test formal hypotheses.
Building on these results, semi-structured expert interviews were conducted to provide explanatory depth and practical interpretation. Interviewees were purposively selected based on professional experience in hospital facilities management, mechanical services engineering or healthcare infrastructure planning. Interview questions focused on the operational feasibility of PdM implementation, including sensor deployment strategies, data reliability, workflow integration and decision-support requirements. Interview data were analysed thematically, with coding informed by survey findings and refined inductively.
Together, the quantitative and qualitative phases provided complementary empirical inputs, enabling observed patterns to be translated into explicit design requirements for the proposed PdM framework. As indicated in Figure 2, outputs from both phases informed the subsequent analytical synthesis, framework development and implementation pathway discussed in later sections.
3.3 Framework development process
The IoT-based PdM framework was developed through a systematic, evidence-based process that integrated quantitative survey findings, qualitative interview insights and established knowledge from the literature. Rather than proposing a purely conceptual model, the framework was designed as a technical–operational architecture intended to guide real-world implementation in hospital settings.
Framework development proceeded in three main steps. Firstly, survey findings were synthesised to identify dominant maintenance practices, levels of digital maturity and key barriers and opportunities shaping PdM adoption. These findings established baseline conditions and constraints that the framework needed to accommodate. Secondly, qualitative interview insights were used to interpret these conditions, highlighting practical considerations related to sensor selection, data reliability, workflow integration and organisational capacity. Thirdly, insights from both empirical phases were mapped onto a layered system structure, defining the functional roles of sensing, data acquisition, analytics and decision-support components within a hospital HVAC context.
This iterative process ensured that the resulting framework was neither technology-driven nor context-blind, but instead reflected the interaction between empirical evidence, expert knowledge and system-level design principles. The framework therefore represents a practice-oriented contribution that bridges PdM theory and hospital facilities management requirements.
4. Results: empirical drivers of framework design
4.1 Organisational readiness outcomes
Organisational readiness emerged as a primary empirical driver shaping the feasibility and design requirements of the proposed IoT-based PdM framework. Readiness was assessed across two dimensions: resource availability (technical, digital and human capacity) and HVAC system criticality, reflecting the operational importance of HVAC systems in hospital environments (Alghanmi et al., 2022; Bokrantz et al., 2020; Lavy and Shohet, 2004).
Survey results indicate partial and uneven readiness for digital maintenance transformation. Preventive maintenance remains dominant, while familiarity with PdM is low and maintenance documentation is largely paper-based or minimally digitised. Limited use of CMMS and BMS platforms suggests weak foundational digital infrastructure across many facilities, reinforcing reliance on manual, experience-driven maintenance decision-making.
In contrast, HVAC systems were consistently identified as highly critical assets due to their roles in patient safety, infection control and service continuity. The coexistence of high system criticality and low digital preparedness reveals a structural readiness gap: hospitals recognise the importance of reliable HVAC performance but lack the organisational capacity to support advanced, data-driven maintenance strategies. This misalignment explains why PdM is perceived as desirable yet difficult to implement in practice.
Prioritisation results further show that relative advantage and compatibility outweigh cost and technical expertise in shaping adoption preferences, indicating openness to PdM when it aligns with existing workflows and delivers clear operational value. However, when considered alongside reported barriers – particularly skills limitations and high initial investment – these findings confirm that organisational readiness mediates whether perceived benefits translate into actionable adoption decisions.
Overall, the results indicate that organisational readiness is necessary but insufficient for PdM adoption. Awareness of HVAC criticality must be matched by minimum levels of digital infrastructure, skills and data governance. These findings justify phased implementation pathways in which digitisation, basic monitoring and capacity building precede advanced predictive analytics.
4.2 Technical and operational insights
Beyond organisational readiness, the findings identified technical and operational conditions that directly shaped the architecture of the proposed framework.
The continued dominance of preventive and corrective maintenance, together with limited PdM familiarity, confirms that hospitals operate in low-data maintenance environments. Under such conditions, advanced analytics are ineffective without reliable data inputs, necessitating prioritisation of foundational sensing focused on a limited set of high-value parameters rather than dense sensor deployment.
Fragmented and largely manual maintenance records constrain immediate use of historical data for predictive modelling and limit interoperability with analytics platforms. This supports the inclusion of a data consolidation layer to enable gradual migration from paper-based records to structured digital logs.
Skills gaps and system heterogeneity further constrain implementation. Maintenance teams often have limited exposure to analytics tools, while HVAC systems typically comprise equipment from multiple vendors. These conditions favour interpretable, rule-based diagnostics and open protocols as entry points rather than opaque predictive models.
Adoption preferences also favour solutions that integrate with existing workflows and demonstrate immediate operational value, reinforcing a decision-support orientation in which PdM outputs inform maintenance actions rather than replace human judgement. Sensitivity to initial cost further underscores the need for scalable, modular system design that supports low-cost entry points such as edge-based monitoring and phased analytics deployment.
Collectively, these insights indicate that PdM success in hospitals depends less on algorithmic sophistication than on alignment with existing maintenance realities. Accordingly, the framework emphasises modularity, interoperability, usability and phased progression.
4.3 Expert validation themes
Expert interviews validated and refined the empirical drivers identified in the survey, while clarifying how PdM can be realistically operationalised in hospital HVAC contexts.
A consistent theme was the need for incremental implementation, with experts emphasising that hospitals are unlikely to transition directly from reactive or preventive maintenance to fully automated PdM. Data quality and trust were also highlighted as critical enablers, with preference for transparent diagnostics and actionable recommendations over black-box models.
Asset prioritisation emerged as a further validation theme. Given resource constraints, experts advised focusing initial PdM deployment on high-risk or high-impact HVAC assets serving critical clinical spaces. Integration with existing maintenance workflows was emphasised to ensure PdM tools complement rather than disrupt established practices.
Finally, experts stressed the importance of capacity building and role clarity, noting that while advanced analytics may be externally developed, hospitals must retain sufficient internal capability to interpret outputs and act on recommendations.
Overall, expert validation confirmed that effective PdM implementation depends on alignment with organisational maturity, operational workflows and risk management priorities. These insights informed refinement of the framework into a practical, phased and context-flexible architecture. Table 2 summarises how empirical findings directly informed key architectural and functional design choices.
5. Proposed Internet of Things-based predictive maintenance framework
5.1 Framework design rationale
The proposed IoT-based PdM framework was developed in direct response to the empirical constraints identified in Section 4, including uneven organisational readiness, fragmented maintenance data, limited digital infrastructure and the need to align with existing hospital HVAC management practices. Rather than assuming readiness for advanced analytics or highly instrumented systems, the framework adopts a phased, modular and system-agnostic design that supports progressive adoption in line with organisational maturity.
The framework is intentionally agnostic to specific IoT deployment models. Depending on data availability, connectivity and institutional capacity, sensing and analytics functions may be implemented using edge-based, fog-based or cloud-based configurations. In resource-constrained hospital environments, edge-based monitoring combined with rule-driven or statistical analytics is often more feasible and operationally resilient, reducing reliance on continuous connectivity and advanced computational infrastructure (Lee and Lee, 2015; Psomas et al., 2021). While artificial intelligence and machine-learning techniques may enhance predictive accuracy at later stages, they are not prerequisites for initial PdM adoption.
Accordingly, the framework is conceived as a functional architecture rather than a prescriptive technology stack, defining how sensing, data acquisition, analytics and decision-support components interact to enable PdM in hospital settings. Emphasis is placed on interpretability, workflow compatibility and incremental capability development, ensuring that PdM augments existing maintenance decision-making rather than requiring wholesale technological transformation.
5.2 Framework architecture
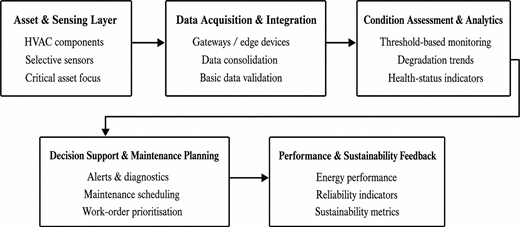
Figure 3 illustrates the layered architecture of the proposed IoT-based PdM framework for hospital HVAC systems, showing the integration of sensing, analytics, decision support and performance feedback. The framework comprises five interrelated functional layers derived from the empirical findings:
Sensing and asset layer Selective monitoring of critical HVAC assets is supported using a limited set of high-value sensors (e.g. temperature, power consumption, runtime and fault status). Asset prioritisation is guided by system criticality rather than blanket deployment, supporting cost control and phased implementation.
Data acquisition and integration layer Sensor data are collected via edge devices or gateways and consolidated into a structured digital repository. This layer accommodates heterogeneous equipment and enables gradual migration from manual or fragmented records to unified digital logs.
Analytics and condition assessment layer Condition monitoring and fault detection are implemented using interpretable rule-based or statistical methods as entry points, with scope for more advanced predictive models as data quality and organisational capacity improve. The emphasis is on early fault identification rather than automation.
Decision-support and maintenance planning layer Analytics outputs are translated into actionable maintenance insights, including alerts, prioritised work orders and scheduling recommendations. Integration with existing maintenance workflows reinforces human decision-making rather than replacing it.
Performance and sustainability feedback layer Maintenance outcomes feed back into system performance tracking, enabling continuous assessment of reliability, energy efficiency and asset condition. This feedback loop supports ongoing performance improvement and alignment with sustainability objectives.
The contribution of the framework lies not in individual technological elements, but in their empirically informed structuring and sequencing. Unlike conventional PdM architectures that assume mature digital infrastructure and immediate readiness for advanced analytics, the framework explicitly accommodates low-data environments, incremental capability development and integration with established maintenance workflows. By embedding performance and sustainability feedback within the maintenance decision loop, maintenance is positioned as an active mechanism for sustaining long-term energy and operational performance rather than a peripheral support function.
6. Interpreting the empirical drivers of the proposed framework
This study developed an IoT-based PdM framework grounded in empirical realities rather than technical idealisations. The findings in Section 4 show that organisational readiness, technical constraints and operational practices jointly shape the feasibility of PdM implementation in hospital HVAC systems. Rather than reflecting resistance to innovation, the results reveal a structural misalignment between the criticality of HVAC systems and the maturity of existing maintenance infrastructures.
The continued dominance of preventive and corrective maintenance, coupled with limited digital documentation, indicates that many hospitals operate in low-data maintenance environments. While this aligns with prior studies on experience-driven decision-making, the present findings extend this literature by demonstrating how such conditions directly determine PdM design requirements. Phased implementation, selective sensing and interpretable analytics therefore emerge as empirical necessities rather than discretionary design choices.
The prioritisation of compatibility and relative advantage over cost and complexity further indicates that PdM adoption is driven by perceived operational fit rather than technological novelty. This reinforces the need to conceptualise PdM for hospitals as workflow-embedded decision-support systems rather than standalone analytics platforms. Collectively, these findings shift PdM discourse from algorithmic performance towards system integration and organisational feasibility.
6.1 Contribution to predictive maintenance and sustainability literature
The proposed framework contributes to PdM literature by integrating maintenance decision-making, energy performance and sustainability feedback within a single functional architecture. Existing HVAC PdM studies largely emphasise fault detection accuracy, predictive modelling or optimisation-based control, offering limited guidance on operational deployment in risk-sensitive environments such as hospitals (Es-sakali et al., 2022; Katipamula and Brambley, 2005; Zonta et al., 2020).
By contrast, this framework responds to calls for systems-level approaches that bridge cyber-physical technologies and facilities management practice. The inclusion of a performance and sustainability feedback layer addresses a recognised gap in both BEATs and MATs, which typically assess environmental performance or asset condition in isolation. From a theoretical perspective, the findings also refine PdM adoption interpretations by showing that organisational readiness mediates the relationship between perceived value and implementation feasibility, particularly in resource-constrained and heterogeneous infrastructure contexts.
6.2 Practical implications and broader relevance
For hospital facility managers, the findings indicate that PdM implementation should prioritise foundational actions – digitising maintenance records, identifying critical assets and deploying a limited set of high-value sensors – before pursuing advanced analytics. Aligning PdM outputs with existing maintenance governance structures is essential, with dashboards and alerts designed to support professional judgement, accountability and service continuity.
Although empirically grounded in hospital HVAC systems, the framework’s architecture is not hospital-specific. The design principles identified are applicable to other energy-intensive and operationally sensitive building typologies, including laboratories, data centres, campuses and commercial buildings. Hospitals function here as a high-risk testbed rather than a limiting case, with the layered, technology-agnostic structure supporting adaptation across contexts characterised by heterogeneous systems, variable digital maturity and constrained maintenance resources.
7. Framework substantiation and implementation pathway
This section explains how the proposed IoT-based PdM framework is empirically substantiated and outlines an indicative pathway for implementation. Consistent with the design-oriented scope of the study, the framework is not performance-tested but derived from analytical synthesis of survey findings, explanatory expert interviews and established PdM and building-systems literature.
Framework substantiation is achieved through direct alignment between empirical findings and architectural design choices. Survey results revealed high HVAC system criticality alongside limited digital maturity, fragmented maintenance documentation and continued reliance on preventive and corrective maintenance. Expert interviews contextualised these findings, highlighting constraints related to data quality, technical capacity, system heterogeneity and workflow integration. These conditions informed a framework structured around phased adoption, selective sensing, interpretable analytics, workflow-integrated decision support and performance feedback.
Each framework layer corresponds to a recurring empirical driver: asset prioritisation reflects system criticality and cost sensitivity; data consolidation responds to fragmented records; interpretable analytics address skills gaps and trust concerns; decision-support integration aligns with existing maintenance practices; and performance feedback captures the link between maintenance actions and energy performance. This correspondence provides the primary empirical substantiation for the framework.
Design coherence and implementation pathway
The framework is internally coherent through explicit sequencing of PdM capabilities in line with organisational readiness. Rather than assuming immediate availability of high-quality data or advanced analytics, it supports incremental progression from basic monitoring to predictive functions. Operational feasibility was prioritised throughout development, with expert insights emphasising usability, accountability and compatibility with existing maintenance workflows. Accordingly, the framework adopts a decision-support orientation and remains technology-agnostic to accommodate heterogeneous HVAC systems and legacy infrastructure.
An indicative three-stage implementation pathway is proposed. The foundational stage focuses on digitising maintenance records, identifying critical HVAC assets, and deploying a limited set of high-value sensors. The functional PdM stage integrates sensor data into a central repository and introduces rule-based or statistical diagnostics to support early fault detection and maintenance planning within existing workflows. The advanced PdM stage involves gradual adoption of predictive analytics and systematic feedback between maintenance actions, energy performance and sustainability indicators, with progression dependent on data quality, skills development and organisational readiness.
Scope and limitations
The framework has not been evaluated through pilot deployment or longitudinal performance testing and therefore does not quantify energy savings, downtime reduction or lifecycle cost impacts. Substantiation is based on evidence from a specific healthcare context, and implementation outcomes may vary across regions and building typologies. The framework should therefore be interpreted as a design-informed and empirically supported architecture that provides a foundation for future implementation and evaluation in hospital and other energy-intensive building environments.
8. Conclusion and implications
This study addressed a critical gap in hospital facility management by developing an IoT-based PdM framework grounded in the organisational, operational, and sustainability realities of hospital HVAC systems. Although PdM technologies are well established in industrial settings, their application in healthcare buildings has remained fragmented and weakly aligned with empirical practice. This study contributes by proposing a framework that is both technically informed and contextually feasible for hospital environments.
The primary contribution is a multi-layered PdM architecture that integrates sensing, data management, analytics, decision support and performance feedback within a single functional structure. Rather than prioritising algorithmic sophistication, the framework emphasises modularity, interpretability and phased adoption, reflecting the uneven digital readiness and resource constraints observed empirically in hospital settings. In doing so, it advances PdM as a decision-support capability aligned with existing maintenance governance rather than as a standalone analytics solution.
A second contribution lies in explicitly bridging maintenance practice and sustainability performance. By positioning maintenance as an active mechanism for sustaining energy efficiency and operational resilience, the framework responds directly to the limitations of existing BEATs and MATs, which largely treat environmental performance and maintenance as separate domains. Methodologically, the study demonstrates how an explanatory sequential mixed-method design can be used not only for interpretation but as a structured input into framework development, ensuring alignment between observed practice and system design logic.
From a practical and policy perspective, the findings highlight the need to reposition maintenance as a strategic component of healthcare sustainability and infrastructure resilience. PdM adoption should prioritise foundational digital capability, data governance, asset prioritisation and workflow integration rather than automation alone. At the policy level, the framework illustrates the value of incorporating digital maintenance readiness and predictive decision support into healthcare infrastructure guidelines and sustainability assessment criteria.
Limitations and future research
The proposed framework is empirically substantiated through analytical synthesis rather than operational deployment and therefore does not quantify energy savings, downtime reduction or lifecycle cost impacts. In addition, the empirical evidence reflects a specific healthcare context, and implementation pathways may vary across regulatory and institutional settings. The framework also focuses primarily on HVAC systems, and other hospital systems may present additional PdM requirements.
Future research should prioritise pilot implementation and longitudinal evaluation to assess operational, energy and reliability outcomes. Further work is needed to explore integration with digital-twin platforms, advanced analytics and hospital information systems as organisational maturity increases. Comparative studies across building typologies and geographic contexts would also support refinement of scalability, transferability and policy relevance.
The first author acknowledges the financial support provided through the University International Postgraduate Award (UIPA) at the University of New South Wales (UNSW Sydney), Australia, which supported his doctoral studies.
Ethics statement
This study was approved as a low-risk human research project by the University of New South Wales Human Research Ethics Committee (Approval No. iRECS8122). All participants provided informed consent prior to participation.