The study aims to provide insights into the availability of common drugs with respect to disease load, regarding three common childhood diseases, acute respiratory infection (ARI), diarrhoea and malaria. The study flags an important issue regarding the level of expertise of the present system to address humanitarian logistics in case of emergency.
A mixed‐method approach using both qualitative and quantitative study techniques was used to collect data. Hospital level data were collected from randomly selected primary health centers and community health centers. a cohort of three community health centers and nine primary health centers were selected for the study. The data collected were both on disease load and availability of drugs during the study period (2009‐2012), using a retrospective cohort. Expert interviews were conducted of practising medical practitioners on classification of drugs into Vital, Essential and Desirable categories.
Results show that the month of September represents the highest morbidity (case loads of all three diseases taken together). Acute respiratory infection is most prevalent among the three diseases, with total case loads of 1,539 cases during the month of September (during 2009‐2012). However the Vital and Essential drugs availability for acute respiratory infection was found to be 7 per cent, 57 per cent for malaria and 98 per cent for diarrhoea. Drug supply was not only inadequate but also uneven and erratic, having weak correlation with the pattern of disease morbidity.
Cases who attended the government‐owned health centres were only considered for the study and it did not consider those who were attended by private practitioners. The study did highlight the capability of the system to manage ongoing health supplies and the extent of vulnerability it can pose in case of any humanitarian crisis but the latter remains outside the scope of the present study.
The study adds to the existing body of literature by demonstrating the gap that exists in availability of drugs against requirement, for common childhood illness. The study provides health policy makers with a useful guide to establish drugs requirement based on disease load, which holds policy implications across other low and middle income countries as well.
Introduction
Drugs are an important input to any health system. It is an unpleasant experience when someone suffering could not have an access to prescribed drugs, either because of unavailability of drugs or because of their unaffordability. Issue of making drugs and essential hospital consumables available in right quality and right pricing has been raised as an important consideration (Mazi Sam et al., 2008). It is already well documented that there is chronic shortage of essential drugs and surplus of non‐essential drugs having little relevance to the morbidity pattern of the area (Gupta and Verma, 2012). Drugs requirements (types, quantity and frequency) are highly context specific, some drugs which are non‐essential in one place may be essential in other places depending on country's disease pattern and level of development (Mazi Sam et al., 2008).
Childhood morbidity and mortality are affected by multiple factors and diseases. More than 6.9 million children under the age of five, die every year globally (World Health Organization (WHO), 2011). More than half of these early child deaths are due to conditions that could be prevented or treated with access to simple, affordable interventions. Leading causes of death in under‐five children are diarrhea, acute respiratory infection (ARI), malaria, pneumonia and preterm birth complications. About 10 percent of all childhood deaths can be attributed to diarrhea, 7 percent to malaria and 9 percent to ARI (WHO, 2011). Availability of essential drugs in adequate quantity, frequency with desired level of quality is crucial to effectively bring down mortality and morbidity at the regional as well as at the global level.
Knowledge and skills of managing an effective and efficient supply chain of essential drugs is essential not only for an ongoing health programme but also extremely important during any kind of emergencies which demands for humanitarian responses. Medical equipment's and drugs are among commonly procured goods by humanitarian agencies during emergencies (Taupiac, 2001) and hence local expertise in effective supply‐chain management is always an asset.
Background
Essential drugs as defined by the WHO are those that satisfy the priority health care needs of the population, they are selected with due regard to public health relevance, evidence on efficacy and safety and comparative cost effectiveness. The idea of essential drugs and establishing a list was developed way back during the world health assembly of 1975, aimed to increase the range and availability of drugs to the population with poor access. Very often the quality of primary health care system is judged by patients on the basis of availability of needed drugs (Mouala et al., 2009). Based on the criticality of diseases, the drugs could be classified into three categories: vital, essential and desirable, commonly known as VED. Unavailability of “vital” drugs could lead to serious functional dislocation of patient care services in hospital even when unavailable for a short period of time. Unavailability of “essential” drugs beyond a few days or a week, the functioning of the hospital can be adversely affected whereas shortage of “desirable” drugs would not adversely affect patient care or hospital functioning even if shortage is prolonged (Devnani et al., 2010).
The paper presented by Gupta (Gupta and Verma, 2012) highlighted that the scenario of drug availability in India is not in short supply but also chaotic. Drugs are found to be of inferior quality, adulterated, poor‐quality tracking, unavailability of VED lists, supply of expired (time) drugs and inadequate budgetary provision are some of the challenges highlighted. The paper further highlights that more than 65 percent of the Indians lack access to essential drugs. About 82 percent of the health expenditure in the country is paid by the people themselves, of which 60 percent are on drugs. There is chronic shortage of essential drugs and surplus of non‐essential drugs, having little relevance to the morbidity pattern of the area or in accordance with the essential drug list (Roy and Jha, 2009). Supplies are erratic and include banned drugs, irrational combinations and hazardous drugs which are readily available and many a times given without supervision (Gupta and Verma, 2012). Storage of drugs has also been identified as one of the major challenges in some of the states in India, leading to delayed supply at the Primary Health Center's (PHC's) and Community Health Centre's (CHC's) (Barik et al., 2011).
Child health care in India is primarily immunization centered, resulting in quite huge spending in the area of immunization. This often leads to insufficient budget allocation to other essential drugs. In most health centres and other Primary health care centers many of the essential drugs remain out of stock, gets exhausted quickly or diverted. Availability of essential drugs constitute the major challenges affecting the sustained availability of essential drugs and supply for Primary Health Care service (Mazi Sam et al., 2008). Issues regarding drugs safety and meeting the expected standards (Mouala et al., 2009) has also been raised in some of the studies. Even if the drugs are available, hardly any of the scientific technique of inventory control (namely vital‐essential‐desirable technique) is applied for maintaining availability of drugs, which needs to be adopted as a routine practice as part of regular supply‐chain management, for optimal use of resources and elimination of out‐of‐stock situations in the hospital pharmacy (Devnani et al., 2010).
However, end users satisfaction and managing cost of services are critical at all level to strength health systems (Colletti, 1994). Patients satisfaction is increasingly being recognized as an appropriate measure for determining how well a particular organization is accomplishing its mission and, while patient's satisfaction surveys provide valuable information and may be used to improve the entire operation of the supply‐chain management (Swinehart and Smith, 2005). Determining the level of care continues to require vigilant scrutiny over the potential cost/benefit analysis and is considered to be vital for the policy makers (Kumar et al., 2009).
This is well accepted that an efficient and effective supply‐chain management can improve availability of VED drugs at all levels. There are suggestions toward improved supply‐chain management and high‐volume purchasing which have benefited other industries. Similar approaches could also reduce health care costs (Agwunobi and London, 2009) but there are apprehensions regarding involvement of private providers in the drug supply chain to bridge down the shortage faced by health services, particularly at the hospital level and demands for deeper understanding (Lopez‐Moreno et al., 2011).
Effective supply‐chain management includes coordination and collaboration with partners, which could be suppliers, intermediaries and third part service providers (Council of Supply Chain Management Professionals (CSCMP), 2009). Effective and interactive communication routes within the supply chain, specifically between users, manufacturers, purchasers and suppliers are crucial at all stages (Browne et al., 2004). Similar functions encompassing range of activities, including preparedness, planning, procurement, transpiration, warehouse, tracking and tracing are vital in case of humanitarian logistics as well (Thomas and Kopczak, 2005). But unlike normal supply chain, humanitarians are always faced with greater degree of unknown (Van Wassenhove, 2006). As one would expect greatest unknowns in any humanitarian logistics are the time, place and severity of a disaster. Any minor fault with respect to its effectiveness or efficiency could literally mean the difference of life and death for the people affected.
The experience and level of expertise that the logisticians within the government managing regular health supply chain is indispensable and would prove to be immensely important whenever there is an outbreak of epidemic or any other situation which calls for humanitarian aids. There is a dearth of logisticians who can plan, assess and coordinate human and material for relief operations (Chikolo, 2006). Lack of clearly defined career pathways has resulted in loss of experienced logisticians, and can have a significant negative effect because experience has been found to be more important that disaster plans (Eriksson, 2009) and there by worsening the situation.
The study proposes to identify and discuss the gap that exists (if any) in availability of drugs against requirement, based on the disease load for three common childhood illness which affects children below five years there by suggesting the strength or efficiency of the ongoing supply‐chain management for common drugs. The study also acknowledges the extent of vulnerability that would emerge in case of any humanitarian assistance, unless the level of expertise that exists with logisticians in managing ongoing and regular supply chain of drugs is god enough. But the latter remains outside the scope of the study.
Methodology
Study design
In order to achieve the stated objectives, cross‐sectional study followed by retrospective cohort study using mixed method (qualitative as well as quantitative) were undertaken. Cross‐sectional study was considered to be the best suited study design as this would give stock position of VED drugs in a single snap shot at that point of time. For the study, Primary Heath Care centers were randomly picked up using simple random techniques and a cross‐sectional studies were undertaken. Based on certain predefined criteria, a group of 31 PHCs and 3 sector level hospitals were selected for the cross‐sectional study, which formed the cohort. A retrospective cohort study was undertaken, considering data of previous three years.
The quantitative study was used to collect secondary data (HMIS and/or Panchavyadhi reports) on disease load of ARI , diarrhea and malaria among children below five years in selected PHC and CHC of Dhenkanal district of Odisha, India and stock position of VED (vital, essential and desirable) drugs.
Expert interviews of selected practitioners were conducted to generate data on standard treatment guidelines; common drugs required for treatment of ARI, diarrhea and malaria. As not much secondary literature could be available with the government on these fronts, which are referred or practiced, relying on expert interviews became indispensable. Expert interviews were conducted to calculate unit requirement of drugs (per patient; per episode) and further classification of drugs into VED categories. The interviews were undertaken in person, administering a predefined semi‐structured questionnaire to capture the data. The semi‐structured questionnaires were further translated into the local language (Odiya) to minimize the language barrier.
Study period
The study was conducted from April 2012 to June 2012. The study considered data from three successive years (2009‐2010, 2010‐2011 and 2011‐2012) in retrospect.
Study setting
The study area was the district of Dhenkanal of the state of Odisha, India. The district was selected based on the technique of simple random sampling in the state of Odisha (Figure 1).
Profile of the government‐supported health care infrastructure at the district:
District Head Quarters – 1 number;
subdivision headquarters Hospitals – 2 number;
area hospital – 1 number;
community Health Center – 8 number;
sector level hospitals – 3 number; and
primary health centers – 31 number.
Study participants
The selections of respondents were based on certain predefined eligibility criteria. Practicing pediatricians, working with the Government of Odisha, India, for not less than five years were considered to be eligible for the study. An informed written consent was taken from all participating respondents for the study.
Sample size
Out of the eight CHCs in Dhenkanal District, three CHCs were selected using stratified random sampling. One CHCs was selected from each of the tribal (Birasal of Kankadahad block), non‐tribal (Odapada of Odapada block) and mixed population of tribal and non‐tribal (Anlabereni of Kamakhyanagar block).
Three PHCs from each of the selected CHCs were selected using a simple random method, making it a total of nine PHC's in total for the study.
The total number of samples selected (three CHCs and nine PHCs), represented about 25 percent of all primary health institutions in the district of Denkanal.
Study tool
A semi‐structured questionnaire was developed and field tested before the actual collection of the data. Along with the semi‐structured questionnaire, few structured tools also were required to collect data on: disease load, drug requirement, drug stock and classifying drugs into VED categories.
In order to estimate requirement of drugs, an average requirement of a drug per patient per episode and approximate percentage of patients requiring the drug, were calculated. Based on units of a drug required per patient per episode and disease load an annual requirement of individual drugs was calculated. The identified drugs were further classified into VED categories.
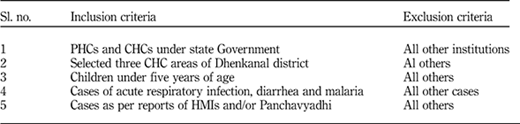
Inclusion and exclusion criteria (Table I)
Ethical consideration
Necessary permission for the study was taken from the ethical committee at the Indian Institute of Public Health, Bhubaneswar. Permission from the chief district medical officer, Dhenkanal district, Odisha, India, for collection and utilization of the data was taken. An informed written consent from respondents for interviewing, recording and utilizing the data provided was obtained. Though this study was undertaken within one of the randomly selected districts of Odisha in India but the research implication holds true, not only for the larger part of India but also for many more regions across the globe which falls under the low‐ and middle‐income countries.
Limitations of the study
The cases who attended the government owned CHC's and PHCs were only considered for the study. There would be cases reported and getting treated at some private health care facilities in the same geography that remained excluded from the study. Also the study considered the availability of drugs till the PHC level. There could be a possibility that all those drugs which were made available at the sub‐center level or with the community health workers as ASHAs (particularly in case of drugs related to malaria), were not taken into consideration in this study which might have led to under‐estimation of drug availability. However, the study being a cross‐sectional study, provides a snap shot of the situation at a particular point of time, which has his own limitations as causality of the association ship could not be established.
The study reflects the availability of VED drugs for common childhood diseases, which could be used as a good proxy to reflect the efficiency and effectiveness of the ongoing health supply chain of the health department. The study did flag the risk of managing logistics in case of any kind of disaster which would need humanitarian assistance, but this remains very much outside the scope of the study.
Results
Case loads
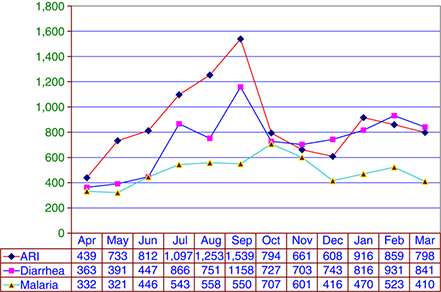
All three diseases (ARI, diarrhea and malaria) taken together contributes to morbidity in the district of Dhenkanal, Odisha (refer to Figure 2). The case load of ARI shows an increasing trend from the month of May (733 cases) onwards stiffly up to September (1,539 cases) and reaching the highest peak in the year. There is sharp decline in the month of October (794 cases) and gradual decrease there after till December (608 cases). In January there is rise in cases followed by slow decline in February and March. Maximum cases are coming from June to September. Diarrhea case load shows a similar trend to that of ARI, with number of cases rising from June (447 cases) to July (866 cases) with a small decline in August (751 cases) and highest number of cases were reported in September (1,158 cases). There is fall in December followed by slow rise up to February. Malaria case loads shows a gradual increase from the month of April (332 cases) till the month of October, when it reaches its highest peak (707 cases) and there after the case load decreases gradually. All the three diseases taken together, shows rise of case loads from the month of June onwards and reaching its peak during the month of September (ARI and diarrhea), where as that of malaria the peak is in the month of October. All three diseases represent a moderate rise during the month of January and February. Case load of ARI is the highest followed by diarrhea and there after malaria. None of the diseases have zero incidences at any point of the year.
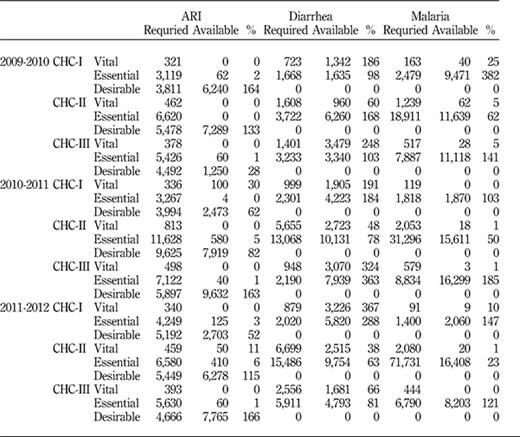
Drug requirement vs availability (Table II)
Vital drugs availability and ARI: with respect to ARI, the vital drugs availability was found to be “zero” across all three selected CHCs in the year of 2009‐2010. Thirty percent availability was recorded at CHC‐I during 2010‐2011 and 11 percent at CHC‐II (2011‐2012) while 0 percent availability was recorded among other CHC during the same period of study (2009‐2012).
Vital drugs availability and diarrhea: in five out of nine instances vital drugs for diarrhea were available more than requirement (more than 100 percent of requirement; in rest four cases it is <100 percent the lowest being in CHC‐II.
Vital drugs availability and malaria: the availability was found to be ranging between 0‐5 percent across all CHCs during the study period (2009‐2012), except for CHC‐I having 25 percent and 10 percent in 2009‐2010 and 2011‐2012, respectively.
Essential drugs and ARI: the availability was found to be ranging between 40‐60 percent among half of the institutions, 0 and 4 percent among two more and more than 100 percent availability has been recorded in three cases.
Essential drugs and diarrhea: this shows availability of 100 percent or more across CHC‐I and CHC‐III. However, in CHC‐II represented 78 percent and 63 percent availability during 2010‐2011 and 2011‐2012, respectively.
Essential drugs for Malaria: more than 100 percent availability has been recorded in six out of nine PHCs. Among two PHCs from CHC‐II (2009‐2010 and 2010‐2011) represented availability of 50 to 60 percent.
Requirement vs availability of all drugs taken together
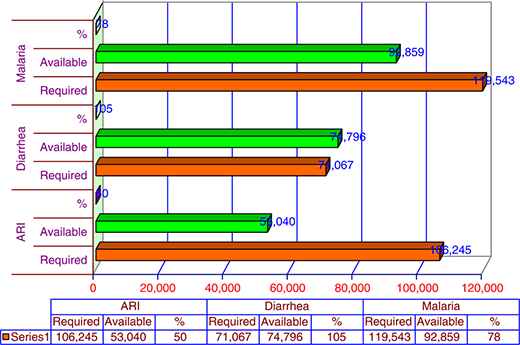
Considering the requirement against availability of all vital drugs taken together during the last three years (2009‐2012), the drugs availability against requirement in case of ARI was found to be 50 percent, 105 percent for diarrhea and 78 percent in case of malaria.
Requirement vs availability of vital and essential drugs (excluding desirable drugs)
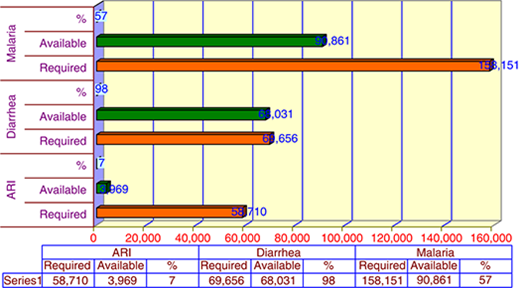
In case of ARI, vital and essential drugs taken together, the availability against requirement was found to be 7 percent, for diarrhea 98 percent and for malaria it was found to be 57 percent, respectively (please refer to Figure 4).
Requirement vs availability of vital and essential drugs (CHC wise)
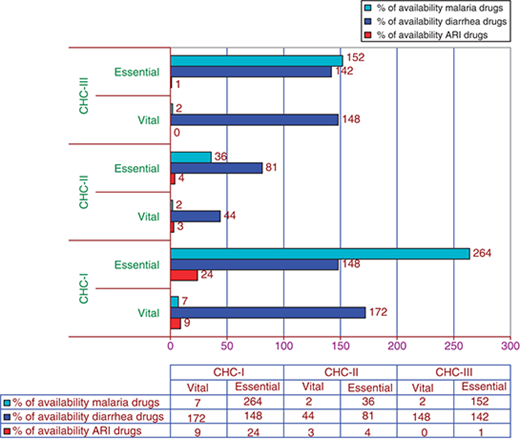
CHC‐I reported 9 percent availability of vital drugs, 24 percent of essential drugs with respect to ARI. Vital and essential drug availability for diarrhea has found to be 172 percent and 148 percent and for malaria 7 percent and 264 percent of vital and essential drugs, respectively.
CHC‐II reported 3 percent and 4 percent availability of vital and essential drugs for ARI. Forty‐four and 81 percent in case of vital and essential drugs with respect to diarrhea and 2 percent of vital and 38 percent of essential drugs were available in case of malaria.
CHC‐III, vital drugs availability for ARI was “nil” and essential drugs was found to be 1 percent. Vital and essential drugs for diarrhea were 148 percent and 142 percent, respectively. For malaria, vital drugs availability was 2 percent and essential drugs were 152 percent, respectively.
Discussion
Disease load
ARI, diarrhea and malaria have shown a high prevalence among the child population in Dhenkanal district with varying intensities across the year. All the three diseases have a rising trend from the beginning of the rainy season, i.e. from June till the month of September, when it reaches its peak. The rainy season being prone to contamination of drinking water sources, poor sanitary conditions of human habitation especially in villages where open field defecation is a practice, a disease friendly environment of hot and wet weather, increased breeding of vectors like mosquitoes and flies, etc. might have favored the increased incidence of all the three diseases. ARI has the highest incidence among other discussed diseases, with the disease frequency of 1,539 cases in the month of September (2009‐2012). Diarrhea falls on the second category, showing a case load of 1,558 during the same period (September). Malaria shows its peak during October, having a disease load of 707 cases (2009‐2012). The period from August to October seem to be the most vulnerable period for children under five years of age so far as these three diseases are concerned. A minor peak of ARI and diarrhea comes during the month of January and February has also been reported. At no point of time any of the diseases has a zero incidence among the study population across the study period (2009‐2012).
Drug availability
The overall availability of all drugs, across all selected CHCs taken together (please refer to Figure 3), reflects availability of drugs with respect to ARI is only 50 percent of requirement, for anti‐malarial drugs it is 78 percent and diarrheal drugs availability was adequate with 105 percent availability of the amount required.
However, the situation reflects a very different picture once we look a little deeper into the issue of availability against requirement. It is alarming to note that ARI having the highest disease load (1,539 cases) reflects poor availability among the three. The vital and essential drugs availability taken together (please refer to Figure 4) the situation paints an alarming picture. The drugs available for ARI was found to be as low as 7 percent, for malaria it was 57 percent and only in case of diarrhea the availability was found to be adequate (98 percent). With both ARI and malaria having such high‐case loads and malaria being a national programme the drug availability is expected to be much better than what the study reflected. The study was restricted to consider the availability of drugs up to the PHC level, availability of drugs which might have been at the levels close to the community (at PHCs or with health workers), would have remained unreported, depicting a little skewed picture.
A deeper analysis of drug availability at individual institutions (please refer Table I) reflects that the vital drugs availability stands at “zero” stock among all three CHCs and also among PHCs. Seven out of the nine selected PHCs stands at “zero” stock availability of vital drugs. Similar is the condition with malaria where vital drugs availability stands at the range of 0‐5 percent availability among seven out of nine PHCs selected for the study. Essential drugs are reflects significant deficient for ARI (0‐6 percent availability) among all categories among the period of the study (2009‐2012). The issue is not just centered about the availability of VED drugs; it is also about the availability of drugs whenever it is required the most. It is well recognized that quantum of drugs would move up as morbidity and/or mortality are on the rise. In contradiction to this the finding says that there is neither uniformity nor equity in drug supply among the CHCs which has been selected for the study (please refer to Figure 5). Some places there are excess supply while deficient in other. ARI is the most neglected disease as far as the drug availability is concerned. Proper estimation of drug requirement as per disease load and reallocation seems to be the emerging key issues which need immediate attention.
The procurement and supply of drugs to the primary health facilities across the country including the state of Odisha are expected to be based on the essential drug list (NELM, 2011).The population norm and the pre‐existing disease pattern forms the basis of calculating requirement of drugs which either overlooks the changes in drug response to a disease that has happened over the period of time or overlooking the existing regional disparity in actual disease load. With large scale investment in health programmes, widening portfolio, increasing volume of products and services to newer population, supply chain must be flexible and responsive to the changing environment (John Snow Inc, 2012). The requirement of categories, volume and timeliness of drugs availability therefore demands a more scientific and need‐based assessment taking the above factors into account.
Nevertheless, the drugs supply and distribution is in a poor state of affair and needs immediate attention. High level of expertise is required to respond to humanitarian logistics management which should preferably come from the existing system, and are missing at present. The logisticians in normal situation are struggling to manage an effective supply chain of health supplies and hence the capability of the logisticians in any kind of epidemic outbreak, which might calls for humanitarian aids is an important question to be answered. The local capacity within the health system might proved to be insignificant in providing leadership or direction in case of any humanitarian crisis and might be heavily dependent on external humanitarian agency to bridge the gap.
Conclusion
ARI, diarrhea and malaria contributes to large number of case loads, across the year in case of children below five years of age. Availability of drugs in adequate quantity, frequency, timeliness with desired standard is important to save lives and respond to any humanitarian crisis. Large number of drugs has been identified through the essential drug list for children for these three killer diseases. However, to understand the importance of these drugs to bridge in morbidity and bringing down mortality, there is a greater need for classification of these drugs into VED. The number of case loads in the case of ARI has been reported to be the highest but during the same time the availability of drugs for ARI was found to be the poorest. Similar situation was recorded for malaria but a much improved status has been reported for diarrhea. September is the most vulnerable month for children with respect to number of cases (all three diseases taken together) and April appears to be comparatively safer (with minimum reported cases). The present study looks at the disease case loads of the three main identified diseases and a comparative analysis of availability of drugs against its requirement (based on disease load), which gives a snapshot of the existing situation of supply chain in the district or at the state level. Considering the study to be a cross‐sectional study, the study was limited to represent association ship and therefore causality could not be established. However, the present study identifies some of the critical gap areas with respect to the capacity of the existing logisticians within the health systems in managing ongoing health supplies and the larger threat that it poses in case of any humanitarian crisis. However, analyzing the extent and level of expertise of the system in managing humanitarian logistics was beyond the scope of the present study and hence calls for further studies, at much larger scale and depth to understand the issues further.