

The aim of this study was to explore the reasons for preferring home as a birth delivery place and identify the socio-economic and cultural factors influencing the choice of delivery place in rural Bangladesh.
The data for the study come from a community-based cross-sectional study conducted among 464 mothers in a rural sub-district of Bangladesh in 2019. Respondents were selected randomly from the frame listing all mothers with inclusion criteria, using a two-stage cluster sampling design. Data were collected through a face-to-face interview. Both descriptive and inferential statistics and logistic regression models were used for data analysis.
The results indicate a very high rate (58%) of home delivery. About 20% mothers never received ANC visit. Preference for home delivery was high (63%). Mothers with no education, aged 30 and above, multi-parity, low wealth status, lack of knowledge about institutional delivery, no or <4 ANC visits, received no advice about the delivery place, no pregnancy complications, decision about health care, and prior plan for home delivery were identified as significant predictors of home delivery. Cost of services, cultural practices and attitude towards health facility, lack of a female delivery assistant, perceived fear of caesarian section, poor quality of services, and lack of knowledge about maternity services appeared as important barriers for institutional delivery.
Based on primary data from a rural area, this study would help understand reasons and factors affecting home delivery and developing an appropriate strategy for the improvement of institutional delivery and maternity care services in Bangladesh.
Introduction
Nearly half a million maternal deaths occur worldwide annually from pregnancy and childbirth-related complications. More than 90% of these deaths occur in developing countries [1]. However, most of these maternal deaths are preventable [2, 3]. The high level of maternal mortality in developing countries has been attributed to poor utilization of maternity services, and partly to the non-availability and accessibility of services [4]. It has been observed that in many developing countries, more than one-third of pregnant women have no access to or contact with health professionals during pregnancy, and more than a half of the deliveries occur without a skilled attendant present [5, 6]. On the other hand, about 98% of women in developed countries receive antenatal care (ANC) services and up to 94% of births are attended by a skilled birth attendant (SBA) [1, 7]. Lack of proper care during pregnancy, delivery and the postnatal period in most developing countries not only increases the risk of maternal and child death but also increases the risk of many severe diseases and disabilities among the mothers [8]. Despite repeated calls and consensus about the importance of antenatal care and delivery at a health facility, the use, and access of maternal health services (MHS) remain low in most developing countries, and delivery of birth at home is widespread [8].
Although Bangladesh, a socio-ecologically vulnerable country of South East Asia, has made some visible progress in the health sector, it is still facing the challenge of a high maternal mortality rate (MMR) [9]. After Sub-Saharan Africa, Bangladesh has the highest MMR in the world, the low utilization rate of pre-and post-natal care, and low access to SBAs [10]. About 42% of births are supported by an SBA, which is quite low in comparison to the global standard of about 80% [11]. Home delivery of pregnancy is still a widespread tradition in Bangladesh. According to the 2014 Bangladesh Demographic and Health Survey (BDHS), 62% of total births still take place at home and 48% of children are born with the help of a traditional birth attendant. Less than one-third of births were attended by doctors [12]. The situation is worse in rural areas. It is, therefore, important to identify the underlying factors responsible for poor utilization of maternity care services and identify the reasons for choosing home delivery in rural Bangladesh. This study examines the factors influencing home delivery among rural mothers in Bangladesh, utilizing primary data obtained through a cross-sectional survey in a rural community.
Methodology
Setting, sample selection and study design
A community-based cross-sectional survey was conducted in a purposely selected rural Upazila (sub-district) namely, Madhupur in Tangail district of Bangladesh. About 296,729 people live in the sub-district [13], who lead a very traditional life with agriculture as the main means of subsistence. Most of the people are illiterate, as the literacy rate is only 31% (7+ years). The majority (90%) of the population are Muslim [13].
The study was conducted under the auspices of the Daffodil International University (DIU), Bangladesh, with financial support from the Bangladesh Medical Research Council (BMRC) – a research and training institute under the Ministry of Health (MoH). The Department of Public Health of DIU implemented the survey.
The study considered mothers who had a live birth within one year of the survey date as the target population. The required sample was determined using the formula [14]:
where n = size of the sample, deff. = design effect (which was taken as 1.5 based on the 2014 BDHS results), p = expected proportion of a specific indicator (in this case proportion of home delivery which was 0.69, according to the 2014 BDHS report), Z = 1.96 at 5% level of significance and d = the level of maximum error deemed acceptable (which was chosen as 0.05). Given the above specifications, Eqn (1) yielded a required sample size of 493 respondents.
The sample respondents were selected following a two-stage cluster sampling approach, considering the catchment area of the 40 Family Welfare Assistants (FWAs) as the cluster. FWAs are government-appointed full-time trained female health workers at the community level. They maintain a list of all the postnatal mothers and children in their catchment area for their routine work. To facilitate the sample selection cost-effectively, we utilized this readymade list of postnatal mothers. It was decided to select 31 respondents systematically from a selected cluster. Thus, it was required to select 16 clusters at random to achieve the targeted sample of 493 respondents. Ultimately, 464 mothers were interviewed, giving a response rate of 94%.
To examine the adequacy of the achieved sample of 464 respondents, a statistical power analysis was done using GPOWER software (version 3.1.1). Post-hoc power analysis with α = 0.05, n = 464, df = 1, and an effect size of 0.15 indicated that our sample would provide a power of 0.90.
The data collection was begun in September-October 2019 with a structured questionnaire. Data were collected through a face-to-face interview by trained interviewers.
Statistical analysis
The study used place of delivery - a binary variable with two categories: home and health-facility – as the outcome variable and the socio-economic, demographic, knowledge, and use of maternity care-related variables as explanatory variables. Both descriptive and inferential statistical methods were used for data analysis. Frequency distribution was used for analyzing the background characteristics of the mothers, pattern of utilization of maternity care by mothers, and reasons for preferring home delivery. Bivariate analysis and Chi-square test were employed for analyzing the association between place of delivery and the characteristics of mothers. A p-value of <0.05 was considered statistically significant. Multiple logistic regression models were employed to identify the significant predictors of home delivery after controlling the relevant confounders. Data were analyzed using Statistical Package for Social Science Software.
Ethical consideration
The study was approved by the Institutional Review Board of the Bangladesh Medical Research Council (BMRC) (Ref. BMRC/HPNSP-projects/2019/185).
Results
Socio-demographic characteristics
Among the 464 responding mothers, nearly sixty percent (59%) were young mothers aged 20–29 years. About 13% of the mothers were in the adolescent group of 15–19 years (Table 1). The average age of the mothers was 25.7 years. Almost half (49%) of the mothers were married before the legal age at marriage of 18 years and 97% were married before 25 years. The average age at marriage was 17.5 years. One-fourth (25%) of the mothers had no formal education. Education was more prevalent among husbands than their wives. Mothers were mostly (95%) housewives. More than one-third (37%) of the mothers were primiparous i.e. first-time mothers. The average family size was about five members. About 43% of the mothers had daily exposure to either radio or television. Most (78%) of the mothers lived at a distance of more than 30 min' walk from the nearest health facility.
Percentage distribution of mothers and percentage of mothers by place of delivery of the last child, according to their background characteristics, Madhupur 2019
| Characteristics | Total n (%) | Place of delivery | ||
|---|---|---|---|---|
| Home n (%) | Health facility n (%) | p-value⋆ | ||
| Total | 464 (100) | 271 (58.4) | 193 (41.6) | |
| Socio-demographic characteristics | ||||
| Age (yrs) | 0.023 | |||
| <20 | 59 (12.7) | 37 (62.7) | 22 (37.3) | |
| 20–29 | 274 (59.1) | 146 (53.3) | 128 (46.7) | |
| 30+ | 131 (28.2) | 88 (67.2) | 43 (32.8) | |
| Mean (SD) | 25.7 (5.7) | 26.1 (6.2) | 25.1 (5.1) | |
| Age at marriage (yrs) | 0.256 | |||
| <18 | 225 (48.5) | 139 (61.8) | 86 (38.2) | |
| 18–24 | 222 (47.8) | 121 (54.5) | 101 (45.5) | |
| 25+ | 17 (3.7) | 11 (64.7) | 6 (35.3) | |
| Mean (Sd) | 17.5 (3.2) | 17.3 (3.3) | 17.8 (3.0) | |
| Level of education | <0.001 | |||
| No education | 117 (25.2) | 86 (73.5) | 31 (26.4) | |
| Primary | 178 (38.4) | 117 (65.7) | 61 (34.3) | |
| Secondary+ | 169 (36.4) | 68 (40.2) | 101 (59.8) | |
| Work status | 0.018 | |||
| Not working (housewife) | 441 (95.0) | 263 (59.6) | 178 (40.4) | |
| Working | 23 (5.0) | 8 (34.8) | 15 (65.2) | |
| Husband's education | 0.002 | |||
| No education | 26 (5.6) | 22 (84.6) | 4 (15.4) | |
| Primary | 185 (39.9) | 116 (62.7) | 69 (37.3) | |
| Secondary+ | 253 (54.5) | 133 (52.6) | 120 (47.4) | |
| Parity | 0.041 | |||
| Primi-parous | 172 (37.1) | 90 (52.3) | 82 (47.7) | |
| Multi-parous | 292 (62.9) | 181 (62.0) | 111 (38.0) | |
| Wealth status | 0.039 | |||
| Low | 188 (40.5) | 123 (65.4) | 65 (34.6) | |
| Medium | 91 (19.6) | 50 (54.9) | 41 (45.1) | |
| High | 185 (39.9) | 98 (53.0) | 87 (47.0) | |
| Family size | 0.998 | |||
| ≤4 | 214 (46.1) | 125 (58.4) | 89 (41.6) | |
| 5+ | 250 (53.9) | 146 (58.4) | 104 (41.6) | |
| Mean (Sd) | 4.9 (1.6) | |||
| Media exposure | 0.488 | |||
| Daily/Regularly | 198 (42.7) | 112 (56.6) | 86 (43.4) | |
| Occasional | 266 (57.3) | 159 (60.0) | 107 (40.0) | |
| Distance to nearest health facility | 0.293 | |||
| ≤30-min walk | 100 (21.6) | 63 (63.0) | 37 (37.0) | |
| >30-min walk | 364 (78.4) | 208 (57.1) | 156 (42.9) | |
| Awareness about maternity care | ||||
| Knowledge of complications at the time of delivery | 0.061 | |||
| Yes: Could mention at least one danger sign | 307 (66.2) | 179 (58.3) | 128 (41.7) | |
| No: Could not mention any danger sign | 157 (33.8) | 92 (58.6) | 65 (41.4) | |
| Aware of maternity services of health facility | 0.019 | |||
| Yes | 362 (78.0) | 204 (56.4) | 158 (43.6) | |
| No | 102 (22.0) | 78 (76.5) | 24 (23.5) | |
| Whether received advice for delivery place | <0.001 | |||
| Yes | 341 (73.5) | 177 (51.9) | 164 (48.1) | |
| No | 123 (26.5) | 94 (76.4) | 29 (23.6) | |
| Having pregnancy complications during last pregnancy | <0.001 | |||
| Yes | 234 (50.4) | 111 (47.4) | 123 (52.6) | |
| No | 230 (49.6) | 160 (69.6) | 70 (30.4) | |
| Preferred delivery place | <0.001 | |||
| Home | 291 (62.7) | 217 (74.6) | 74 (25.4) | |
| Hospital | 173 (37.3) | 54 (31.2) | 119 (68.8) | |
| Prior plan for delivery place of last birth | <0.001 | |||
| No plan | 94 (20.3) | 63 (67.0) | 31 (33.0) | |
| Home | 209 (45.0) | 162 (77.5) | 47 (22.5) | |
| Health facility | 161 (34.7) | 46 (28.6) | 115 (71.4) | |
| Decision on health care | 0.042 | |||
| Self/Self and husband | 247 (53.2) | 122 (49.4) | 125 (50.6) | |
| Husband | 127 (27.4) | 80 (63.0) | 47 (37.0) | |
| Others | 90 (19.4) | 52 (57.8) | 38 (42.2) | |
Note(s): ⋆p-values are based on the Chi-square test
Awareness and utilization of maternity care
About one-third (34%) of the mothers had no idea of any danger signs such as artificial rupture of amniotic membrane, a newborn with a respiratory problem, excessive bleeding, swelling and tearing of uterus, and so on, while 22% were not aware of maternity services. Half (50.4%) of the mothers reported that they had some pregnancy complications with their last pregnancy. The majority (62%) of mothers preferred to deliver their babies at home. One-fifth (20%) of mothers had no prior plan for the delivery place of their last baby, while 35% had a prior plan to deliver at a health facility and 45% had a prior plan to deliver at home (Table 1).
About 80% of the mothers had at least one ANC visit; half (50.4%) of them had 1–3 visits, while 30% had at least four visits and nearly 2% had completed the WHO recommended minimum of at least eight ANC visits [8]. On average, mothers received less than 3 visits (Figure 1). Of those who received ANC visits, most of them (56%) received services from medically trained providers: 38% from doctors and 18% from a nurse, family welfare visitor (FWV), and community health workers. About 71% of mothers received ANC services from public health facilities. Nearly sixty percent (58%) of mothers delivered their last child at home and 42% in the health facility.
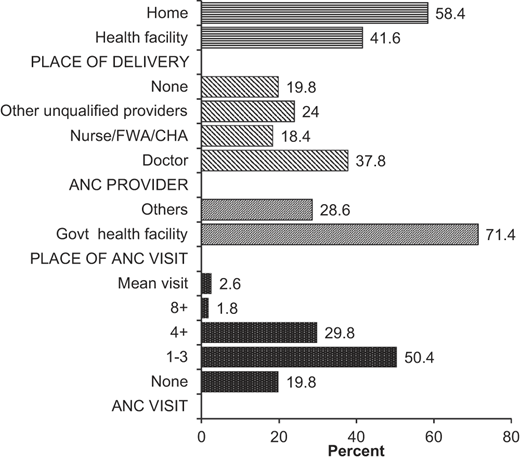
Distribution of mothers according to the pattern of utilization of ANC and delivery care, Madhupur 2019
Distribution of mothers according to the pattern of utilization of ANC and delivery care, Madhupur 2019
Reasons for preferring home delivery
The two most prominent reasons for preferring home delivery were low or no cost involved in-home delivery (51%), and feeling comfortable with home delivery as they could get relatives to take care of them and maintain their privacy (49%) (Table 2). Other important reasons for preferring home delivery included that there was no fear of surgery during a home delivery, no likelihood of an unnecessary caesarian section (CS), no injection used in a home delivery (28%), it was the husband/family member's choice (15%), the delivery was assisted by a female (11%), there were no pregnancy complications (10%) and that they did not know of any alternative place of delivery (9%).
Percentage of mothers according to reasons for preferring home delivery and barriers of delivering at a health facility, Madhupur 2019
| Reasons for preferring home delivery* (n = 291) | Number | % |
|---|---|---|
| Feel comfortable at home as there are relatives to support and privacy is maintained | 143 | 49.1 |
| Lack of money: home delivery is inexpensive | 148 | 51.0 |
| At home, there is no need to fear surgery or unnecessary CS, or injection | 80 | 27.5 |
| Choice of husband/family members | 44 | 15.2 |
| Delivery assisted by a female | 32 | 11.2 |
| Can return to household chores early | 25 | 8.6 |
| Preferred because there was no complication | 29 | 10.0 |
| Don't know where to go for delivery | 27 | 9.3 |
| Others | 17 | 5.8 |
| Major barriers of delivering at a health facility* (n = 291) | ||
| Poor communication | 31 | 10.7 |
| Too far | 22 | 7.6 |
| Unnecessary cesarean | 86 | 29.6 |
| Family members discourage | 127 | 43.6 |
| Lack of female service provider | 52 | 17.9 |
| Expensive | 157 | 54.0 |
| Poor quality of service | 80 | 27.6 |
| Lack of knowledge about delivery care in health facility | 54 | 18.6 |
| Others | 9 | 3.1 |
Note(s): *Involved with multiple responses
Mothers also put forward many barriers to delivering birth in a health facility. The most prominent barriers included the high cost of services at a health facility (54%), followed by the influence of the husband and other family members to deliver at home (43%) (Table 2). Other important barriers to using a health facility included the perceived concept of unnecessary CS done in a health facility (30%), poor quality of services (28%), lack of knowledge about services in a health facility (19%), lack of female service providers (18%) and poor communication (11%).
Predictors of home delivery
The results of the bivariate analysis as presented in Table 1 revealed that mother's age, level of education, work status, parity, wealth status, husband's education, knowledge about maternity services, pregnancy complications, preference for a delivery place, receiving advice for a delivery place, prior plan for delivery place and decision about health care have significant associations with home delivery. However, all the above-mentioned associations provide an unadjusted effect, because the bivariate analysis does not control the confounding effect of other factors.
To get the adjusted effect of a factor after controlling the effect of other confounding factors, multiple logistic regression models were employed, where the adjusted effect of a factor was measured by the adjusted odds ratio (AOR), Table 3. The model was fitted with only significant factors observed in bivariate analysis.
Multiple logistic regression analysis results showing adjusted odds ratios (AORs) of factors associated with home delivery, Madhupur 2019
| Factors | B | SE of B | p-value | AOR | 95% CI of AOR |
|---|---|---|---|---|---|
| Age (yrs) | |||||
| <20 | 0.309 | 0.500 | 0.511 | 1.36 | 0.522–3.698 |
| 20–29 (ref) | 1.00 | ||||
| 30+ | 0.686 | 0.402 | 0.036 | 1.98 | 1.090–4.371 |
| Level of education | |||||
| No education | 1.481 | 0.372 | <0.001 | 4.40 | 2.121–9.122 |
| Primary | 0.472 | 0.329 | 0.151 | 1.60 | 0.842–3.056 |
| Secondary+ (ref) | 1.00 | ||||
| Work status | |||||
| Not working (housewife) | 0.329 | 0.601 | 0.591 | 1.39 | 0.425–4.486 |
| Working (ref) | 1.00 | ||||
| Husband's education | |||||
| No education | 0.292 | 0.646 | 0.651 | 1.34 | 0.377–4.754 |
| Primary | 0.207 | 0.649 | 0.750 | 1.23 | 0.345–4.390 |
| Secondary+ (ref) | 1.00 | ||||
| Parity | |||||
| Primi-parous | 1.00 | ||||
| Multi-parous | 0.766 | 0.289 | 0.008 | 2.15 | 1.220–3.793 |
| Wealth status | |||||
| Low | 0.345 | 0.302 | 0.041 | 1.41 | 1.157–2.892 |
| Medium | 0.174 | 0.325 | 0.592 | 1.19 | 0.630–2.248 |
| High | 1.00 | ||||
| Aware of maternity services | |||||
| Yes | 1.00 | ||||
| No | 0.412 | 0.378 | 0.028 | 1.45 | 1.120–2.758 |
| Antenatal care visit | |||||
| None | 0.788 | 0.345 | 0.012 | 2.20 | 1.132–3.124 |
| 1–3 | 0.356 | 0.265 | 0.043 | 1.43 | 1.096–2.183 |
| 4+ (ref) | 1.00 | ||||
| Whether received advice for delivery place | |||||
| Yes | 1.00 | ||||
| No | 0.412 | 0.399 | 0.024 | 1.50 | 1.112–2.857 |
| Having pregnancy complications during last pregnancy | |||||
| Yes | 0.788 | 0.249 | 0.002 | 2.20 | 1.349–3.583 |
| No (ref) | 1.00 | ||||
| Decision on health care | |||||
| Self/Self and husband | 1.00 | ||||
| Husband | 0.623 | 0.354 | 0.038 | 1.86 | 1.093–3.728 |
| Others | 0.413 | 0.324 | 0.203 | 1.51 | 0.801–2.850 |
| Preferred delivery place | |||||
| Home | 1.00 | ||||
| Hospital | 0.768 | 0.278 | 0.006 | 2.15 | 1.251–3.714 |
| Prior plan for delivery place of last birth | |||||
| No (ref) | 1.00 | ||||
| Home | 1.057 | 0.375 | 0.005 | 2.87 | 1.379–5.999 |
| Health facility | −0.659 | 0.315 | 0.057 | 0.51 | 0.279–0.960 |
Logistic regression analysis identified the following significant predictors of home delivery, namely, maternal age (≥30 years), level of education (no education), parity (multipara), low wealth status, lack of knowledge about maternity services, no antenatal care visit, or <4 ANC visits, receiving advice for a delivery place, the decision of women using health care, having no pregnancy complications, home as the preferred delivery place and prior plan for home delivery.
Mothers aged 30 and above had nearly two times higher odds of having a home delivery than the young mothers aged 20–29 years (AOR = 1.98, 95% CI: 1.09–4.37). Mothers with no education had more than four times higher odds of delivering at home compared to mothers with a secondary or above level of education (AOR = 4.40, 95% CI: 2.12–9.12). Multiparous mothers were about two-times more likely to deliver at home than those with first-time pregnancy (i.e. primiparous) (AOR = 2.15, 95% CI: 1.22–3.79). Mothers from households with low wealth status had 1.41 times higher odds of delivering at home compared to mothers with high wealth status (AOR = 1.41, 95% CI: 1.16–2.89). Mothers with no knowledge about maternity services had a 1.45 times higher risk of delivering at home than those who had knowledge (AOR = 1.45; 95% CI: 1.12–2.76). Mothers with no history of ANC visit had more than two times higher odds of delivery at home than those who had four or more ANC visits (AOR = 2.20; 95% CI: 1.13–3.12). Mothers who could decide on health care independently or jointly with their husbands were found to have 86% less risk of delivering at home, compared to mothers who depended on their husband and other family members for a decision about health care (AOR = 1.86, 95% CI: 1.09–3.73). Mothers who had no pregnancy complications had more than two times higher odds of home delivery than those with pregnancy complications (AOR = 2.20, 95% CI: 1.35–3.58). Mothers who preferred home as the delivery place had more than two times higher odds of home delivery than their counterparts.
Discussion
This community-based cross-sectional study in a rural area of Bangladesh presents the current scenario of maternity care utilization pattern in rural Bangladesh and explored the underlying factors influencing the choice of home as a delivery place among rural mothers. One in every five mothers (19.8%) in this study never received any antenatal care visits. Despite high coverage (80%) of at least one ANC visit, the average number of the visit was found to be less than three visits, which is far below the WHO recommended minimum requirement of four or more visits, or the more recently updated recommendation of at least eight visits for a positive pregnancy outcome [8]. The low average frequency of ANC visits among the study population is an indication of the poor quality of the ANC services in the study area. In order to reduce the risk of adverse pregnancy outcomes, pregnancy complications, and maternal mortality, it is crucial to follow the WHO guidelines of the increased number of ANC contacts, starting with the first ANC visit within the first trimester of pregnancy [8]. These study findings revealed that the target was still far-reaching in rural Bangladesh.
More than half (58%) of the mothers chose home as a delivery place, which is less than the observed rate of 69% in the 2014 BDHS in rural Bangladesh [11]. The recent improvement in the institutional delivery in the country might be related to its recent progress in terms of economic, educational, and social transformation [15].
This study identified many significant predictors of preferring home delivery among mothers living in rural Bangladesh. These include maternal education, age, parity, wealth status, knowledge about maternity care, antenatal care visit, the decision about health care, pregnancy complications, preference for a delivery place and prior planning for the delivery place.
Home delivery was found to be more common among mothers with no education. The finding is consistent with the previous studies in Bangladesh [16], and in neighboring countries such as India [17] and Nepal [18], and also in Ethiopia [19]. The association between women's education and utilization of maternal health services is instinctively sensible, as educated women tend to be more aware of personal health issues, have higher self-efficacy, and are more inclined to self-care and healthy behavior [20]. Contrary to other studies, this study did not find a significant association between choice of delivery place and husbands' education and work status of mothers. These factors may be confounded with other factors.
Mothers aged 30 and above and multiparous mothers were found to have higher odds of home delivery. These findings are similar to the findings of other studies [18, 21]. Mothers with higher age and parity might be less educated and less aware of the advantage of institutional delivery or have less knowledge about modern health care services, and thus, are more likely to deliver at home. On the other hand, a young and primiparous mother might be more educated and thus know the importance of institutional delivery.
Home delivery was found to be more common among mothers from households with poor economic status. More than half of the participating mothers reported financial constraints as one of the most prominent reasons for choosing home delivery as it is inexpensive. On the other hand, the out-of-pocket cost of services in a health facility was mentioned as one of the major barriers to utilizing a health facility. The findings are supported by previous studies in Bangladesh [16, 22], India [23], and Nepal [18]. Studies in Bangladesh demonstrated that, for various reasons, there is a tremendous increase in the cost of seeking hospital obstetric care, limiting the access of poor and middle-class families to modern health care facilities [9, 22, 24].
A mother's knowledge about maternity care services, the experience of pregnancy complications, and utilization of ANC services appeared as significant predictors of choice of delivery place. Similar findings were reported in other studies [25–27]. Mothers who had regular ANC visits likely received information and advice about pregnancy-related complications and the advantages of giving birth at health facilities. Findings also confirmed that mothers who received advice for a delivery place were less likely to have a home delivery.
This study found a significant association between women's decisions on health care utilization and place of delivery, which is consistent with the findings of previous studies [26, 28]. A substantial proportion of mothers reported that they preferred home delivery because their husbands and other family members were in favor of home delivery and against institutional delivery. This is a cultural barrier for Bangladeshi women in both rural and urban areas. Culturally, most Bangladeshi women are highly dependent on their husbands and in-laws for decisions regarding their daily activities including, finance, food, and health care [29]. As expected, a mother's preference for home delivery as well as a prior plan for delivery at home also appeared as significant predictors of home delivery.
This study also identified some reasons for preferring home delivery and major barriers to limit pregnant women from delivering at health facilities. The main reason for preferring home delivery was economic. Out of pocket cost of services, cultural practices and attitudes towards health facilities, the ability to decide on the choice of place of birth, the non-availability of a female delivery assistant in a health facility, the perceived unnecessary CS in health facility, the poor quality of services at a health facility and the lack of knowledge about maternity services were mentioned by the mothers as important barriers to delivery at a health facility. In rural areas, poor road communication and lack of proper transportation also acted as barriers for seeking institutional delivery care [22, 30]. Although Bangladesh has made some progress in achieving some of the health-related goals, the health system of the country still faces many challenges such as a lack of public health facilities, scarcity of skilled workforce, inadequate financial resource allocation, corruption, inefficiency and political instability [31, 32]. The country also has an acute shortage of nurses, medical technologists and allied health professionals such as physiotherapists, laboratory assistants and x-ray technicians [32].
Conclusion
As the reduction of maternal mortality and improvement of maternal and child health largely depends on the proper utilization of ANC services and delivery at health facilities, improving the rate of institutional delivery and attaining adequate numbers of ANC visits should be the key strategy for the maternal and child health program in Bangladesh. One rapid action could be the free arrangement for institutional delivery for poor and rural area mothers, which has already been proved effective in neighboring Nepal [25]. Educating mothers and increasing the awareness of their spouses and in-laws regarding the benefits of institutional delivery could be important areas of intervention to encourage institutional deliveries. Similarly, ensuring the adequate number of ANC visits in compliance with the WHO guidelines and advocating for mothers about institutional delivery during each visit will help improve the rate of institutional delivery. In the long run, promoting female education, poverty reduction and quality of services of the health facilities, particularly in rural areas, would improve maternal health in Bangladesh.
Conflict of Interest: None
The authors are indebted to the participants. Special thanks are extended to the Research Assistants for their tremendous effort in collecting quality data from the field.Funding: This research received funding from the Bangladesh Medical Research Council (BMRC) under the World Bank Research Program.
