

Mental well-being is associated with positive outcomes throughout the life course. This study aims to examine interventions delivered by allied health professionals (AHPs) to alleviate community stressors adversely impacting public mental health and well-being.
Review inclusion criteria comprised experimental and qualitative process evaluations of public mental health interventions delivered by AHPs. Electronic searches in Cinahl, Embase, Medline, PsycINFO and the Cochrane Library, were combined with grey literature searches of National Institute for Health and Care Excellence public health guidance. A narrative synthesis and the Effective Public Health Practice Project appraisal tool were used to evaluate the evidence.
A total of 45-articles were included in the review describing AHP-delivered interventions addressing social disadvantage, trauma, bullying, loneliness, work-related stress, transitional stress, intersectionality, pain and bereavement. No articles were identified evaluating interventions delivered by operating department practitioners or orthoptists. A conceptual map was developed summarising the stressors, and a typology of public mental health interventions defined including: place-based interventions, discrete/one-off interventions, multi-component lifestyle and social connector interventions and interventions targeting groups at risk of mental health conditions.
Many mental health conditions begin in childhood, and a strength of the review is the life course perspective. A further strength is compiling a compendium of public mental health outcome measures used by AHPs to inform future research. The authors excluded many articles focussed on clinical interventions/populations, which did not meet review inclusion criteria. While playing a key role in delivering public mental health interventions, clinical psychologists are not defined as AHPs and were excluded from the review, and this may be construed a limitation. Given heterogeneity of study designs and interventions evaluated numerical analyses of pooled findings was not appropriate.
The review highlights the breadth of community stressors on which AHPs can intervene and contribute in public mental health contexts, stressors which correspond to those identified in UK Government guidance as currently important and relevant to address. The findings can inform developing community public mental health pathways that align with the UK National Health Service (NHS) Long Term Plan, on prevention and early intervention to protect community mental health and well-being. Further can inform the NHS strategic direction for AHPs including informing ways of increasing utilisation of core AHP skills to optimise contributions in public mental health agendas.
It is surprising there were not more AHP delivered evaluations of interventions for other stressors important to address in public mental health settings, for example gambling, domestic violence or that used digital technology, and these are areas for future research. Future research should identify the most active/effective dimensions of multi-component interventions which could be informed by frameworks to guide complex intervention development. The relative paucity of research identified, highlights the predominant focus of research to date on interventions for clinical mental health conditions and populations. The lack of preventative approaches is evident, and an important area for future research to align with UK health and social care priorities.
The review highlights AHP-delivered interventions impacting diverse community stressors across the life course. The findings can inform developing public mental health pathways aligned with government health service priorities to protect mental health and well-being, prioritise prevention and early intervention and increase utilisation of AHP skills across public mental health settings.
Introduction
Mental illness is a leading cause of global disease burden (Vigo et al., 2016; Vigo et al., 2019) and a recent report identified mental health conditions as the second most leading cause of years lived with disability (McDaid et al., 2022). Mental health is defined by the World Health Organisation as a state of well-being, in which individuals realise their abilities, learn/work productively, cope with life’s stresses, contribute to communities (WHO, 2022) and is associated with better outcomes across the life cycle (Campion, 2019). One in six UK adults report having a common mental health disorder (OHID), and a priority of the UK National Health Service (NHS) is developing a preventative approach towards mental illness (NHS; NHSE).
Public mental health approaches comprise prevention (early treatment, relapse prevention), promotion of mental health/well-being and early intervention (Campion, 2019). The determinants of public mental health are multi-facetted, and understanding the complex layers, interactions and interconnections between different health, social and broader contexts is important for guiding interventions (Eriksson et al., 2018; Prince et al., 2007). For example, experiencing poverty, socio-economic disadvantage and inequality are examples of community stressors that heighten risk of mental illness, while mental illness can lead to deprivation through exposure to further community stressors such as lost employment, damaged relationships and stigma (Knifton and Inglis, 2020). In some population groups risk of mental illness is elevated, for example depression and anxiety among people living with cancer (Niedzwiedz et al., 2019), and common mental health disorders among young pregnant women (Estrin et al., 2019). A recent framework identified 55 determinants of public mental health across four levels: individual, family, community and structural (Dykxhoorn et al., 2022). While a recent review of community-based interventions for promoting mental health among older adults defined intervention types including direct and connector interventions, gateway services and systems approaches to intervention (Lee et al., 2022). Key priorities for public mental health commissioning and practice include delivering interventions addressing diverse sectors and community stressors, for example pressure in the workplace and bullying in schools (Campion, 2019). Examples of public mental health interventions found effective include physical activity for subjective well-being (Wiese et al., 2018) and self-help skills for depression among people with physical health conditions (Matcham et al., 2014).
This review examined public mental health interventions delivered by allied health professionals (AHPs). There are 14 AHPs in the UK NHS (Online Supplementary materials: Table OS1). Regulated by professional councils they provide holistic care across the life course, focussing on prevention and improving health and well-being in diverse settings, for example education, work, voluntary, health, social and independent sectors (NHSE). UK guidance for the strategic development and direction of AHP services highlighted under-utilisation of AHP skills within public health agendas and the importance of maximising their potential and contributions (NHSE, 2022). The review was commissioned to inform strategic direction of UK AHP public mental health services provision however we are confident the findings have relevance internationally. The aim of the review was to identify and map:
the stressors impacting public mental health across diverse sectors and populations; and
AHP-delivered interventions to address the stressors and evidence of impact on mental health/well-being.
Finally, to develop a conceptual map summarising the findings.
Method
Study design
The review was reported according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021) (PROSPERO registration: CRD42021295880).
Literature searches were conducted in 2022 for experimental and qualitative process evaluations of public mental health interventions delivered by AHPs. Review inclusion criteria are shown in Table 1. Electronic database searches of Cinahl, Embase, Medline, PsycINFO and the Cochrane Library, were combined with grey literature searches of National Institute for Health and Care Excellence public health guidance. The search strategy included combinations of the following:
Review inclusion and exclusion criteria
| Participants | Adults and children |
|---|---|
| Intervention | Public mental health interventions delivered by AHPs |
| Comparator | Another or no intervention |
| Outcome | Changes in public mental health indicators (e.g. scores on standardised measures, reduced services use) and measures of acceptability |
| Study design | Experimental and qualitative process evaluations of public mental health interventions |
| Exclusion | Exploratory qualitative studies; clinical interventions; no outcome measure relevant to public mental health |
public mental health keywords (e.g. prevention, early intervention, mental well-being, social connectedness/isolation, resilience, positive mental health);
AHP keywords; and
intervention keywords (e.g. programme).
The Medline search strategy is shown in Figure OS2. Articles were sifted at title and abstract then 20% of full texts independently appraised by two reviewers; disagreements were discussed until consensus was reached.
The Effective Public Health Practice Project appraisal tool was used to evaluate risk of bias in quantitative studies (www.ephpp.ca/quality-assessment-tool-for-quantitative-studies/), and the Critical Appraisal Skills Programme checklist for risk of bias in qualitative process evaluations (www.casp-uk.net/casp-tools-checklists/). Quality appraisals were not used to decide which articles to include or exclude from the review, rather the appraisal tools were used to inform interpretation of findings reported in each included study, for example that there was no control group which may have introduced bias.
Data were synthesised narratively in four phases (Popay et al., 2006): a theoretical approach was defined, information extracted from articles was tabulated, comparisons across studies were made and a formal assessment of bias completed. The approach was informed by UK Government public mental health priorities, and previous reviews of public mental health determinants and interventions (Campion, 2019; Dykxhoorn et al., 2022; Lee et al., 2022). The findings were summarised in a conceptual map.
Stakeholder engagement/consultation
We consulted an online meeting of the Public Health Strategy Board representing UK AHP professional bodies regarding aspects of the study and contacted AHP networks for advice on any articles they were aware of.
Results
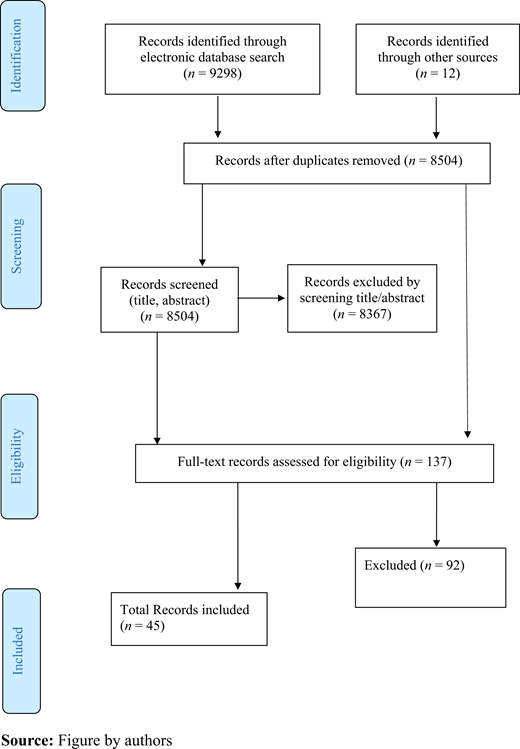
A total of 9,298 articles were identified in the searches; 8,504 after removal of duplicates. A total of 137 articles were evaluated at full text, and 45 selected for inclusion in the review (Figure 1). The references for articles included in the review are shown in the online supplementary materials (OS6). Bias assessments are shown in Table OS4, and outcome measures used in studies to assess change in mental well-being are shown in Table OS5. A total of 15 studies had an overall low risk of bias; most studies used at least one structured outcome measure to assess changes in mental well-being, and 22 studies used a randomized controlled trial (RCT) design. Study characteristics and findings are shown in Tables OS2-3.
Place-based interventions at individual and organisation level: in the workplace
Eight studies evaluated place-based interventions (those delivered in a specific location for example in the workplace, or in higher education), most aimed at developing self-help/care skills, and delivered at individual and organisational level in emergency, palliative, intensive and dementia care workplaces. Five studies were RCTs, focussed on work-related stress. Stress and positive coping improved following osteopathic manipulation in emergency responders (n = 9) (Abraham et al., 2021). After music therapy there were significant improvements in mental well-being among workers on sick leave (Beck et al., 2015), and in stress, fatigue and coping-style among intensive care nurses (Ozgundondu and Metin, 2019). Significant improvements in emotional exhaustion were shown in palliative care workers after art therapy (Ho et al., 2021), and among dementia carers receiving a physiotherapist-delivered psycho-education and relaxation intervention (Barbosa et al., 2015).
Palliative care staff were confident in their ability to access support/supervision after an occupational therapist-led workplace resilience strategy (Apostol et al., 2021), and self-efficacy and perceived support improved among a single cohort of university employees receiving physiotherapist-delivered health coaching (Bezner et al., 2017). Finally, distress was significantly reduced among trauma-exposed mental health professionals receiving art therapy (Segal-Engelchin et al., 2020). The latter three studies, however, lacked a comparator group so risk of bias was elevated.
Place-based interventions to develop self-help/care skills: community, education and workforce training settings
Socio-economically disadvantaged parents showed significant improvements in mental well-being e.g. reduced irritability after music therapy (Nicholson et al., 2008), and there were improvements in resilience among children experiencing trauma after art therapy (Sitzer and Stockwell, 2015). However, both studies lacked a control group so again there was some risk of bias.
Four studies evaluated interventions delivered in vocational training settings. An RCT evaluating physiotherapist-delivered training for physiotherapy trainees, demonstrated significant increases in resilience and positive emotions; the wait-list control was a study strength (Mejia-Downs, 2020). In a small study (n = 14) evaluating mindfulness for radiography trainees, positive non-significant changes in mental well-being were shown (Clarkson et al., 2019). A short music therapist-delivered intervention for a cohort of music therapy students showed significant decreases in stress, anxiety and personal vulnerability (Fiore, 2018). Resilience among trainees improved three-months after a paramedic-developed self-guided resilience resource but was un-sustained six-months later (Vaughan et al., 2020).
Of two community delivered RCTs recruiting children, inattention reduced after art therapy (Malboeuf-Hurtubise et al., 2021) and anxiety significantly reduced after an occupational therapy group intervention (Tokolahi et al., 2018). A strength of the latter study was the wait-list control, all participants accessing the intervention.
Discrete interventions delivered to individuals
Five studies, including four RCTs evaluated discrete (“one-off”) interventions delivered to individuals. In three studies evaluating the effectiveness of insoles/orthoses delivered by podiatrists and orthotists; some improvements in sleep and function were shown but no significant change in mental well-being (Burns et al., 2006; Rasenberg et al., 2021; Wrobel et al., 2015). This was possibly because the primary outcome was pain/function, with mental well-being a secondary outcome measured (in two studies) using the 36-Item Short-Form Health Survey (SF-36) which focusses on general health. Sleep significantly improved in university students after an osteopathic intervention; the RCT design was a strength but the sample size (n = 28) possibly limited representativeness (Wiegand et al., 2015). Finally, acceptability and positive change in affect were demonstrated after virtual reality art therapy for trauma, however, the within-group design potentially introduced bias (Frewen et al., 2020).
Multi-component lifestyle interventions
In three RCTs of occupational therapist-delivered interventions for adults experiencing age-related changes, significant improvements in role/social functioning, emotional and mental health were demonstrated (Clark et al., 2001, 1997, 2012). A physiotherapist-delivered multi-component exercise intervention for adults (average age: 79.5 years) demonstrated cognitive, emotional and social networking improvements in a strongly designed study (Tarazona-Santabalbina et al., 2016).
Design limitations may have introduced bias in the next five studies. A multi-component obesity intervention delivered to a cohort of adults by dietitians and physiotherapists, significantly improved mental health (Batsis et al., 2021). A “healthy habits” occupational therapy program for university students, significantly improved well-being, self-compassion and growth mind-set (Hunt and Coombes, 2021). An 8-months occupational therapist-delivered life-style programme for a cohort of adults experiencing age-related changes showed upward trends in quality of life (Mountain et al., 2008), and participants described benefits to mental well-being, e.g. improved perspective (Chatters et al., 2017). Finally, adults >65 years of age, showed significantly improved mental health and positive trends for psychological well-being, after an occupational therapy health promotion intervention although between-group differences were non-significant (Johansson and Björklund, 2016).
Interventions for groups with elevated risk of mental health conditions
Seven studies evaluated interventions for groups with elevated risk of developing mental health conditions (pregnant and ethnic minority women, veterans, older adults and students). Three RCTs evaluated physiotherapist-delivered exercise programmes during pregnancy; a reduction in depression was demonstrated in two studies (Robledo-Colonia et al., 2012; Songøygard et al., 2012) while the third study with low risk of bias showed no impact on mental well-being (Gustafsson et al., 2016). An exercise programme delivered to a single cohort of Somali women resulted in no change in quality of life, though acceptability was good (e.g. “we exercise, and have fun together”) (Thulstrup et al., 2021). A multi-modal art/music therapy suicide prevention intervention for veterans, reduced suicidal ideation, depression and hopelessness (Vitale et al., 2021). A qualitative evaluation of AHP-delivered workshops on depression and dementia delivered to 1100 adults demonstrated acceptability (e.g. “I liked the information on coping with stress”) though impact on intent to act to improve mental well-being was less evident (Susman et al., 2006). Finally, while art therapy for university students was acceptable there was no impact on indicators of mental well-being (Pizarro, 2004).
A further six studies evaluated interventions for children from groups with elevated risk of mental health conditions; stressors included intersectionality, trauma, bullying, loneliness and bereavement. Of these, two RCTs evaluated the impact of speech therapy (Mallick et al., 2018) and art therapy on bullying (Yan et al., 2019); however, significant reductions in bullying were only demonstrated in children after art therapy (Yan et al., 2019). The art therapy study assessed mental well-being with several outcome measures (Yan et al., 2019), while the speech therapy study used one outcome measure so some effects may have been missed (Mallick et al., 2018). Improved self-concept after art therapy was demonstrated in refugee and immigrant children in a study with low risk of bias (Rousseau et al., 2005). Positive but non-significant changes in depression (Hilliard, 2001) and significantly reduced grief were shown in bereaved children after music therapy (Hilliard, 2007), however both studies were quasi-experimental with moderate risk of bias. A suicide prevention programme for indigenous children, resulted in positive changes in affect pre/post-intervention (e.g. 57% reported moving from stressed to happy) (Doll and Brady, 2013); however, the outcome measure lacked reliability data, and there was no control group.
Social connectors
Two studies evaluated social connector interventions; emotion-focused coping increased significantly after paramedic-facilitated peer support groups on work-related stress for trainees (Pinks et al., 2021). A study strength was using multiple outcome measures. Finally, adolescents’ self-concept improved and loneliness decreased after drama therapy, though the non-randomised design potentially introduced bias (Orkibi et al., 2017).
A conceptual map was developed summarising community stressors, public mental health interventions addressing the stressors and the AHPs delivering them (Figure 2).
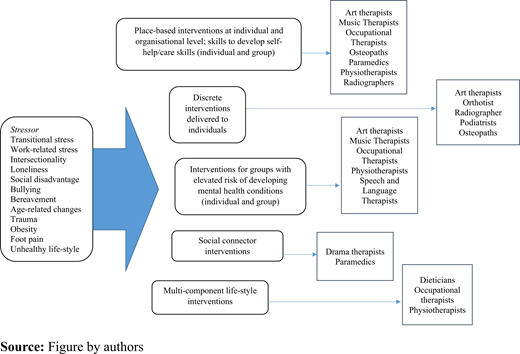
Conceptual map showing stressors addressed, intervention type and AHPs delivering them
Conceptual map showing stressors addressed, intervention type and AHPs delivering them
Discussion
The review has identified a broad range of AHP-delivered interventions addressing diverse community life course stressors in the public mental health domain. The stressors the AHP-delivered interventions aimed to address included trauma, transitional stress, social disadvantage, intersectionality, bereavement, bullying, loneliness, work/age-related stress, pain, obesity and unhealthy lifestyles. Intervention types included:
place-based (delivered at work, school, higher education);
discrete interventions for individuals;
multi-component lifestyle interventions;
interventions targeting groups with elevated risk of mental illness; and
social connectors.
Tables OS2–3 show which articles addressed each stressor area and intervention type.
The community stressors identified in the review that AHPs intervened upon, correspond to those prioritised for intervention in UK Government guidance. This includes mental health support for school children [Department for Education (DfE), 2018]; 11 studies reviewed evaluated interventions for children targeting trauma, transitional stress, social disadvantage, intersectionality, bereavement, bullying and loneliness. Bullying is a priority for intervention (Campion, 2019), as is loneliness, and promotion of social connection via for example social prescribing (Drinkwater et al., 2019; NHSE; RCOT). A priority of the NHS Long Term Plan is transforming perinatal mental health services; three studies reviewed evaluated interventions during pregnancy (Gustafsson et al., 2016; Robledo-Colonia et al., 2012; Songøygard et al., 2012). Suicidality is a mental health priority (NHSHEE; OHID), and the review identified AHP-delivered interventions for suicidality in children and veterans (Doll and Brady, 2013; Vitale et al., 2021).
A multi-layered approach is described as most appropriate to understand the determinants of public mental health, and to guide intervention design and delivery (Campion, 2019; Dykxhoorn et al., 2022; Eriksson et al., 2018). In some of the studies reviewed, multi-component interventions facilitated addressing multi-layered determinants of public mental health, though not without challenges, including identifying the most active/effective components, and resources, for example some interventions were delivered over several months (Mountain et al., 2008). Some interventions were delivered collaboratively between different AHPs; dietitians and physiotherapists delivered an intervention for obesity (Batsis et al., 2021), and physio/occupational and speech and language therapists delivered workshops for dementia and depression-related stressors (Susman et al., 2006). This highlights the potential to address the multi-layered determinants of public mental health through merging the unique skills-sets offered by different AHPs (Dykxhoorn et al., 2022; Susman et al., 2006). This is especially appropriate where intersectionality for example obesity, ethnicity and gender (Thulstrup et al., 2021) compounds community stressors. The determinants of public mental health interconnect across broad contexts (Dykxhoorn et al., 2022; Eriksson et al., 2018) and importantly the review identified interventions overlapping different settings and sectors. For example, mindfulness was evaluated for trainee radiographers (Clarkson et al., 2019), and health coaching for university employees (Bezner et al., 2017), bridging public mental health and occupational health.
Strengths, limitations and future research
Many mental health conditions begin in childhood, and a strength of the review is the life course perspective (Kessler et al., 2007), a further strength is compiling a compendium of mental health outcome measures used by AHPs that can inform future research. While the review area was broad and a scoping review may have been used, a study strength is completing a systematic review allowing mapping the evidence and answering a specific question. We excluded many articles focussed on clinical interventions/populations, which did not meet review inclusion criteria. While playing a key role in delivering public mental health interventions, clinical psychologists are not listed in NHSE’s definition of AHPs and were excluded from the review, and this may be construed a limitation. Given heterogeneity of study designs and interventions evaluated it was not appropriate to complete numerical analyses of pooled findings. The intention was to capture international literature; however, the search terms used the UK NHSE’s titles for AHPs, and articles evaluating public mental health interventions delivered by practitioners working as AHPs in other countries but with different professional titles may have been missed. AHPs do not always have the same roles and regulatory requirements in different countries. In the UK, an AHP is broadly speaking a postgraduate, registered and regulated health professional who has usually been trained to work in the health system during the pre-registration period. This may not always be the case in countries where AHPs have different definitions.
Future research should identify the most active/effective dimensions of multi-component interventions which could be informed by frameworks to guide complex intervention development (Skivington et al., 2021). It is surprising there were not more AHP delivered evaluations of interventions for other stressors important to address in public mental health settings, for example gambling, domestic violence or that used digital technology, and these are areas for future research. The relative paucity of research identified, highlights the predominant focus of research to date on interventions for clinical mental health conditions and populations. The lack of preventative approaches is evident, and an important area for future research to align with UK health and social care priorities.
Conclusions
The review highlights the breadth of community stressors on which AHPs can intervene and contribute in public mental health contexts, stressors which correspond to those identified in UK Government guidance as currently important and relevant to address. The findings can inform developing pathways that align with the UK NHS Long Term Plan, on prevention and early intervention to protect community mental health and well-being. Further, the findings can inform the NHS strategic direction for AHPs including informing ways of increasing utilisation of core AHP skills in order to optimise contributions in public mental health agendas.
Acknowledgements
The authors are grateful to the Office for Health Improvement and Disparities for funding the study. The authors are grateful to Linda Hindle for comments on the manuscript and facilitating consultation with the UK AHP Public Health Strategy Board; and to Joe Lester, Psychology Assistant, Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust, for assisting with data analysis. During the review Eileen Kaner was Director of the National Institute for Health Research Applied Research Collaboration North East and North Cumbria and supported by a NIHR Senior Investigator award. Sarah Wigham was funded by a NIHR ARC NENC Mental Health Fellowship during write-up for publication.
Conflict of interest: None to declare.
Author contribution statement: Simon Hackett, Sarah Wigham, Jane Bourne and Eileen Kaner were awarded funding. Sarah Wigham, Data analysis, Conceptualisation, Writing – Original draft, Writing – Reviewing and Editing. Simon Hackett – Data analysis, Conceptualisation, Writing – Reviewing and Editing. Jane Bourne – Data analysis, Conceptualisation, Writing – Reviewing and Editing. Eileen Kaner – Conceptualisation, Writing – Reviewing and Editing. Kanar Ahmed – Conceptualisation, Writing – Reviewing and Editing.
References
Further reading
Supplementary materials
The supplementary materials of this article can be found online.
