General practice or family medicine has evolved into a cornerstone discipline in undergraduate medical education, reflecting the rising demand for community-based, patient-centred care. This narrative review explores current general practice curriculum models globally and identifies practical strategies for developing and updating curricula to meet evolving healthcare needs.
A comprehensive search across PubMed, Scopus, ERIC and Google Scholar was conducted, adhering to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines for article selection and assessment, to identify core themes, educational principles and innovative approaches to curriculum design and delivery in general practice education from 2005 to 2025.
Of the 700 articles identified, 42 articles included in the final analysis. The review identified five key themes in current general practice curricula: (1) Core competencies (patient-centred care, problem-solving, holistic care and interprofessional collaboration), (2) Targeted regional needs (rural health, marginalised populations and climate health), (3) Clinical placements (early exposure and community-based placements), (4) Educational strategies (blended learning, case-based and interprofessional education) and (5) Teaching and student support (faculty development, infrastructure and student services).
This is particularly timely as medical schools globally are currently undertaking curriculum reviews with a stronger focus on general practice.
This narrative review highlights essential elements for responsive, evidence-informed general practice curricula and suggests ways clinical educators can align teaching practices with evolving community health priorities. Ensuring structured clinical placements and addressing underserved populations are critical to preparing future ready general practitioners.
Introduction
General Practice or Family Medicine is a cornerstone of healthcare systems worldwide. As defined by WONCA Europe, General Practice is recognised as an independent academic discipline with its own educational content, research foundation, and clinical activities focused on the community (Simmenroth et al., 2020; Cole et al., 2020). General practice takes a holistic approach to patient care, addressing the continuum of both acute and chronic health needs, making it indispensable to healthcare delivery.
The College of Family Physicians of Canada proposes four core principles of Family Medicine:
Skilled clinician.
Community-based practice.
Serving a defined practice population.
Emphasis on the doctor-patient relationship (The College of Family Physicians of Canada, 2008).
These principles reflect the central role of family physicians in delivering comprehensive, patient-centred care. Similarly, in 2018, the Royal College of General Practitioners (RCGP) recommended restructuring general practice curricula to focus on core principles rather than specialised knowledge. This shift was aimed at promoting a deeper understanding of foundational content, improving generalist competencies, and enhancing the quality of care delivered (Royal College of General Practitioners, 2018). While these recommendations are being progressively integrated into RCGP training pathways, comparable emphasis on core competencies are found in frameworks such as CanMEDS in Canada and the WONCA Europe (Simmenroth et al., 2020; The College of Family Physicians of Canada, 2019).
The CanMEDS framework, developed by the Royal College of Physicians and Surgeons of Canada, outlines the key roles a general practitioner (GP) must fulfil, including medical expert, communicator, collaborator, leader, health advocate, scholar, and professional (The College of Family Physicians of Canada, 2019). These roles are essential in shaping the broad competencies required for modern general practice, ensuring that GPs are equipped to navigate the increasingly complex healthcare environment.
However, despite ongoing efforts by healthcare systems and educational institutions to train and recruit more GPs, the growing and ageing population, coupled with the increasing complexity of patient needs, has significantly strained the availability of primary care physicians (Central Statistics Office, 2023). Yet, demand for primary care continues to exceed supply, resulting in limited access to healthcare (Duong and Vogel, 2023; Department of Health and Social Care, 2021). Projections from Canada and Ireland indicate a growing shortage of primary care physicians, with healthcare systems struggling to keep pace with increasing demand (Government of Canada; Committee on the Future of, 2017). Similarly, the United States and Australia are facing significant shortfalls, with an estimated deficit of between 20,200 and 40,400 primary care physicians projected by 2036 (GlobalData Plc., 2024; Australian Government Department of Health and Aged Care, 2024). This growing shortage highlights the urgency of continuously evolving general practice curricula to meet the demands of a changing healthcare landscape and ensure the preparedness of future generations of GPs (Royal College of General Practitioners, 2019). In Ireland, this discussion is especially pertinent as medical schools are presently engaged in significant curriculum reviews, many of which are incorporating an increased emphasis on General Practice as part of a broader shift towards community-oriented education.
This narrative review aims to explore current general practice curriculum models, identify regional educational needs, and explore evidence-based strategies to ensure curricula remain adaptable, responsive, and relevant to both global and local healthcare challenges.
Methods
Study design
This narrative review was conducted as informed by Ferrari et al., (2015) (Ferrari, 2015). A literature search was conducted in May 2025 using PubMed, Scopus, ERIC, and Google Scholar. The search focused on identifying studies, curriculum documents, and policy papers that examined models of undergraduate General Practice education published between 2005 and 2025. The objective was to identify core themes, educational principles, and innovative approaches to curriculum design and delivery at a global level.
A structured search strategy was developed using relevant keywords (see Figure 1). Studies were also identified through other sources which included publicly available curriculum documents, and institutional reports. To ensure diverse perspectives, selected studies were purposefully identified through hand-searching reference lists, consultation with subject-matter experts, and review of policy frameworks and institutional resources. This approach enabled the inclusion of academic literature, educational reports, and curriculum guidelines that together provide a comprehensive view of undergraduate medical education internationally.
Two reviewers independently screened all studies. The first reviewer conducted an initial screening of titles and abstracts, followed by a secondary screening by the second reviewer. Full-text records were retrieved and reviewed by both the reviewers when eligibility was unclear or required further assessment. Records that met the inclusion criteria were jointly reviewed, and data extraction was performed collaboratively.
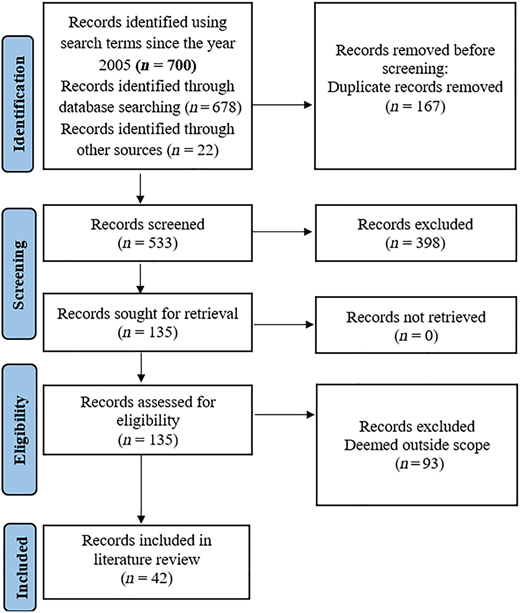
In total, 700 records were initially identified, of which 167 were duplicates and subsequently excluded. After screening, 135 full-text records were assessed, with 42 ultimately meeting all the inclusion criteria for this review (see Figure 2). The selection process followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Inclusion criteria
Articles, reviews, or policy reports discussing the structure, principles, or implementation of undergraduate general practice curricula
Publications from 2005 onwards, to reflect recent trends and developments.
Records addressing curriculum development, pedagogical approaches, assessment strategies, or role competencies in undergraduate general practice education
Exclusion criteria
Records focused solely on non-primary care medical specialities
Non-English publications.
Records without substantive discussion on curriculum content or educational framework or pedagogical approaches
Results
The literature search yielded 700 records. After removing 167 duplicates, 533 records remained for title and abstract screening. Following this preliminary review, 135 full-text records were assessed for eligibility. Of these, 42 records met the predefined inclusion criteria and were selected for final analysis (see Figure 2: PRISMA flowchart).
Characteristics of included studies
The final set of 42 records comprises a diverse range of peer-reviewed articles, curriculum documents, and institutional reports from across multiple countries including Australia (Maley et al., 2009; Royal Australian College of General Practitioners, 2022; Newbury et al., 2005; Royal Australian College of General Practitioners; An Australian Government Initiative, 2022; Hudson et al., 2011), Canada (The College of Family Physicians of Canada, 2008; The College of Family Physicians of Canada, 2019; Students learning medicine in general, 2016; College of Family Physicians of Canada, 2020; Curran et al., 2007; Keegan et al., 2017; Bilodeau et al., 2010; Parson et al., 2019), the United Kingdom (Royal College of General Practitioners, 2018; Royal College of General Practitioners, 2019; Kulkarni and Dua, 2023; Willcocks et al., 2013; Bartlett et al., 2016; Dotchin et al., 2010; Kirtchuk and Markless, 2024; Kennedy et al., 2021; Lee et al., 2014), Malaysia (Malaysian Medical Council, 2020), Ireland (Ravichandran et al., 2025), Bosnia and Herzegovina (Murray et al., 2020), the United States (Tenny and Varacallo, 2024; Zink et al., 2008; Theobald et al., 2022), New Zealand (Mayer and Renouf, 2016; Poole et al., 2010; Shelker et al., 2014), Germany (Kötter et al., 2023), the Netherlands (Ottenheijm et al., 2008), Croatia (Vrdoljak, 2012), the United Arab Emirates (Sulaiman et al., 2024), Iraq (Al-Dabbagh and Al-Taee, 2005), Israel (Benbassat and Baumal, 2012), Namibia (Malan et al., 2024), Mexico (Hamui-Sutton et al., 2017), two from Europe overall (Simmenroth et al., 2020; Global Consortium on Climate and Health Education, 2024) and one focussing on both Canada and Australia (Students learning medicine in general, 2016) (see Table 1). These papers reflect a broad international perspective on undergraduate General Practice education, encompassing diverse healthcare systems, curriculum models, and educational strategies.
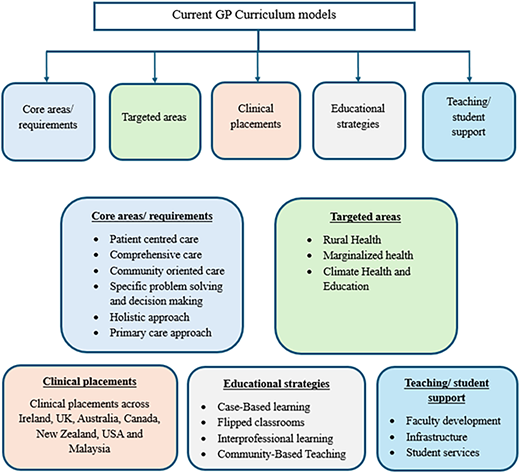
The review revealed five key themes in current general practice curriculum models (Figure 3):
Core Areas/Requirements – Essential competencies and knowledge.
Targeted Needs – Addressing regional and population-specific healthcare needs.
Clinical Placements/Exposure – Hands-on learning in primary care settings.
Educational Strategies – Approaches for teaching and assessment.
Teaching and Education Support/Facilities – Resources supporting both educators and learners.
- 1.
Core Areas/Requirements in General Practice Curriculum
The review revealed the following sub-themes in core areas:
- a.
Patient-Centred Care
The core curriculum should focus on doctor-patient relationships, continuity of care, patient empowerment, and individualised approaches (Simmenroth et al., 2020; Royal College of General Practitioners, 2019; Students learning medicine in general, 2016). Curriculum should prioritise symptoms over diseases, reflecting primary care where patients often present with undifferentiated symptoms (Simmenroth et al., 2020; Royal College of General Practitioners, 2019; Students learning medicine in general, 2016). Students must learn to address common symptoms in family practice, interpret health problems within a broader context. They should consider the family as both a resource and a potential source of health issues (Simmenroth et al., 2020; Royal College of General Practitioners, 2019; Students learning medicine in general, 2016). Communication skills (Simmenroth et al., 2020; Royal College of General Practitioners, 2018) that respect cultural health beliefs and explore social determinants of health should be emphasised (The College of Family Physicians of Canada, 2019). Generalism is vital for patient-centred care, involving a broad foundation of knowledge and skills (College of Family Physicians of Canada, 2020).
- b.
Population Centred Care
The curriculum should involve comprehensive care that addresses acute and chronic conditions while also emphasising prevention and health promotion (Simmenroth et al., 2020; The College of Family Physicians of Canada, 2019). Students must learn to apply population health principles in general practice, including managing multimorbidity and polypharmacy, which are increasingly common in ageing populations (Royal College of General Practitioners, 2018). These competencies should extend to promoting sustainable healthcare practices and tackling inequalities by understanding and addressing social determinants of health (Simmenroth et al., 2020; Royal College of General Practitioners, 2018; Malaysian Medical Council, 2020). Engagement with community health initiatives and public health interventions should be built into undergraduate curricula, helping students connect clinical encounters with broader population-level health concerns. Population-centred care in modern practice also requires proficiency in IT systems, including electronic records, patient safety monitoring, and clinical governance (Simmenroth et al., 2020; Royal College of General Practitioners, 2018; Malaysian Medical Council, 2020). These digital and organisational competencies underpin quality improvement in primary care and support integrated care across different health sectors.
- c.
Specific Problem-Solving and Decision-Making Skills
Students should manage early, undifferentiated disease stages and unique cases that don't fit textbook guidelines (The College of Family Physicians of Canada, 2008). Student-training should include recognising multimorbidity, applying epidemiological reasoning in day-to-day decision-making, selective gathering and interpreting information from history-taking, physical examination, and investigations (Simmenroth et al., 2020; Royal College of General Practitioners, 2019) and rational prescribing, particularly in the context of polypharmacy (The College of Family Physicians of Canada, 2019).
- d.
Holistic Approach
The curriculum should prepare students to recognise that healthcare extends beyond biological disease models to encompass psychological, social, cultural, and existential dimensions (Simmenroth et al., 2020; Royal College of General Practitioners, 2018; Royal College of General Practitioners, 2019). Lifestyle medicine including diet, physical activity, alcohol use, smoking cessation, and stress management should be included as a targeted area of the general practice curriculum (Simmenroth et al., 2020; Royal College of General Practitioners, 2018; Malaysian Medical Council, 2020). Poor lifestyle behaviours are well-documented contributors to chronic disease burden and adverse outcomes, while general practice has demonstrated a strong record in implementing effective behavioural change interventions. Embedding lifestyle medicine and health promotion within undergraduate teaching equips future GPs with the skills to address modifiable risk factors and support patients in achieving better long-term health outcomes (Simmenroth et al., 2020; Royal College of General Practitioners, 2018; Royal College of General Practitioners, 2019).
- e.
Communication skills
Effective communication within healthcare teams is foundational, particularly in general practice settings where patient interactions are central. Communication skills should be horizontally integrated into the curriculum and revisited before clinical clerkships (The College of Family Physicians of Canada, 2019; Royal College of General Practitioners, 2019; College of Family Physicians of Canada, 2020; Malaysian Medical Council, 2020). Research indicates that structured communication modules based on the Calgary-Cambridge model, improve empathy and history-taking in students (Hastings, 2024).Additionally, use of simulated patients or volunteer outpatients have shown to enhance students' ability to manage complex consultations and deliver bad news effectively (Adnan, 2022).
- f.
Interprofessional skills
Interprofessional education (IPE) fosters collaboration among healthcare students from multiple disciplines, promoting team-based approach to patient-centred care. Implementing IPE in curriculum can improve communication, mutual respect and understanding of roles within healthcare system (Mohammed et al., 2021). A medical leadership competency framework is recommended to develop leadership and management for doctors in the context of primary care (Willcocks et al., 2013).
- g.
Research skills
Research skills are a core competency for medical students. Undergraduate curriculum should include training in understanding clinical studies, conducting literature reviews, critical appraisal of scientific research, and translational research. Elective competencies may involve biostatistics, qualitative methods, proposal writing, and scientific publication (Malaysian Medical Council, 2020). Delivering short term research education programmes might be beneficial (Ravichandran et al., 2025). Understanding the principles of Evidence-Based Medicine (EBM) is essential (Simmenroth et al., 2020; The College of Family Physicians of Canada, 2019; Vrdoljak, 2012) and serves as a critical component of the medical profession (Murray et al., 2020). Evidence is categorised into six different levels based on its quality and reliability (Murray et al., 2020; Tenny and Varacallo, 2024).
- h.
Primary Care Approach
The curriculum should prioritise care coordination, patient advocacy, and training students to serve as the first point of contact in the healthcare system (Simmenroth et al., 2020). Emphasis on continuity of care, cost-effective practices, and a thorough understanding of general practice models is essential (Royal College of General Practitioners, 2018).
- 2.
Targeted Areas in General Practice Curriculum
This review highlights several curriculum areas that are particularly important for addressing the unique needs of specific regions and populations.
- a.
Rural Health
Approximately one-third of Australians reside in rural areas, where access to healthcare is limited and social isolation is common (Maley et al., 2009; Royal Australian College of General Practitioners, 2022). Rural medical education programmes have been offered for undergraduate medical students in Australia to address healthcare challenges in rural communities (Maley et al., 2009). Initiatives like the “rural week” immersion in curriculum have shown promising shifts in student attitudes toward Indigenous health and rural practice (Newbury et al., 2005). In New Zealand, rural exposure begins in the second or third year of medical school, with placements ranging from two to six weeks (Mayer and Renouf, 2016). Programmes like the Rural Medicine Immersion Programme offer year-long rural training and mentorship, offering students sustained clinical and community engagement (Poole et al., 2010; Shelker et al., 2014). In the United States, the Rural Physician Associate Programme delivers longitudinal, immersive learning experiences that foster progressive clinical skill development under consistent mentorship (Zink et al., 2008). Similarly, in Canada, the majority of medical schools require or offer rural placements as either mandatory or elective components of undergraduate education (Curran et al., 2007). In England, comparable placements in rural general practice have been well-received, with students and educators reporting that long-term local learning benefits both trainees and their host communities (Bartlett et al., 2016).
- b.
Marginalised health
The 2022 Aboriginal and Torres Strait Islander Health Curriculum Framework provides guidance for undergraduate health professional education aiming to reduce health inequities stemming from socioeconomic factors such as income, education, and employment (An Australian Government Initiative, 2022). Australia's increasingly diverse population, 29.8% of whom were born overseas also includes over 90,000 asylum seekers as of 2021 (Royal Australian College of General Practitioners, 2022). In response, the curriculum integrates content on migrant, refugee, and asylum seeker health to better prepare future clinicians for these roles (Royal Australian College of General Practitioners).
- c.
Planetary Health and Education
Climate change is emerging as a core concern in modern medical education. Its impacts on respiratory, cardiovascular, and mental health are being increasingly addressed in curricula. Integrating planetary health into general practice curricula equips future clinicians with the knowledge and skills to address the health impacts of environmental changes (Moore, 2021). Stellenbosch University School of Medicine in Africa has incorporated planetary health modules into the medical curriculum (Stellenbosch University).
The European Network on Climate and Health Education (EnCHE) collaborates with medical schools in the UK, Belgium, and France to integrate climate-related content, equipping students to advocate for sustainable healthcare and contribute to net-zero health systems (Global Consortium on Climate and Health Education, 2024). A recent study by Kötter et al. (2023) found that students strongly support the inclusion of planetary health and environmental medicine in medical education, advocating for longitudinal integration throughout training (Kötter et al., 2023). Expanding these modules to encompass public and global health such as health surveillance and policy could enhance their overall impact and relevance (Dotchin et al., 2010).
- 3.
Clinical placements
Early clinical exposure is critical for student engagement and skill development. Attaching medical students to general practices in the community at an early stage of their education can foster professional attitudes and promote independent learning (Kulkarni and Dua, 2023). Ideally, this should begin during the preclinical years through patient interactions and community-based placements. Such exposure enhances motivation, fosters clinical reasoning, and helps students manage ambiguity and uncertainty (Simmenroth et al., 2020; Students learning medicine in general, 2016; Malaysian Medical Council, 2020; Ottenheijm et al., 2008). Clerkships should ideally provide at least three months in a single family medicine setting, integrated into community practice for 12 months or more ideally (The College of Family Physicians of Canada, 2008). WONCA Europe suggests at least 12 weeks of exposure to clinical placements for GPs (Simmenroth et al., 2020). These immersive models support continuity of care and strengthen students' relationships with patients and supervisors.
Longitudinal Integrated Clerkships (LICs), where students provide continuous care to patients across multiple disciplines, are particularly effective. They support competency development through sustained relationships with patients and mentors, fostering communities of practice that enhance clinical learning and interprofessional collaboration (Kirtchuk and Markless, 2024).
Clinical placement durations and formats vary widely across institutions and countries, depending on curricular design, healthcare system integration, and local priorities. While licencing bodies often set baseline standards, few provide specific mandates on the duration of placements. Key barriers to clinical placements include difficulty securing sites due to insufficient qualified preceptors, physician burnout, time constraints, and increasing numbers of medical students (Hudson et al., 2011; Theobald et al., 2022).
Below are a few publicly available examples of undergraduate medical clinical placements from leading institutions worldwide, illustrating different settings (see Table 2).
- 4.
Educational Strategies (Teaching and assessment)
Preferred educational strategies combine experiential learning with flexible, evidence-informed pedagogical approaches:
- a.
Case-Based Learning: Development of symptom-focused capstone cases tailored to local health needs can improve diagnostic and clinical reasoning skills (Keegan et al., 2017; Kennedy et al., 2021).
- b.
Flipped Classrooms: Students engage with complex clinical scenarios such as multimorbid patients prior to class, allowing for active problem-solving and peer learning during contact hours. The integration of e-clinics enhances these experiences (Simmenroth et al., 2020; Sulaiman et al., 2024).
- c.
Interprofessional Learning: Collaborative learning with colleagues from geriatrics, pediatrics, surgery, and allied health fields enhances team-based care and communication skills (College of Family Physicians of Canada, 2020; Kirtchuk and Markless, 2024). Interactive, small-group learning aligned with Knowles' principles of adult education further strengthens this approach (Bilodeau et al., 2010; Raffing et al., 2023).
- d.
Community-Based Teaching: General practice placements in the early years of study are the most common form of community-based education (Lee et al., 2014). Additional strategies include patient home visits and community immersion (Al-Dabbagh and Al-Taee, 2005).
- e.
Early special commitment: A 2012 study suggested that early commitment to a medical speciality could streamline training, align curricula with future job requirements, and improve physician workforce planning (Benbassat and Baumal, 2012).
- f.
Other Strategies: The use of clinical cards, virtual patient cases, peer teaching, and open-access learning platforms also contributes to learner engagement and skill acquisition (Keegan et al., 2017).
- g.
Assessment Approaches: Effective assessment strategies are multidimensional. They should include written and oral evaluations, objective structured clinical examinations, practical attachments, small group assessments (The College of Family Physicians of Canada, 2008), and electronic portfolios for performance tracking and reflection (Royal College of General Practitioners, 2018; Malan et al., 2024).
Competency-based assessment frameworks, including Entrustable Professional Activities (EPAs), are increasingly used to guide feedback and evaluate learners' readiness for practice (Simmenroth et al., 2020; Hamui-Sutton et al., 2017). The University of Ottawa's Continuing Professional Development (CPD) office has also proposed a 12-step framework to map these competencies into educational programmes (Parson et al., 2019).
- 5.
Teaching/Student support
a. Faculty Development: Institutions should bridge the gap between generalist and specialist educators through CPD accreditation, teaching networks, and support for academic roles at community sites (College of Family Physicians of Canada, 2020).
b. Infrastructure: Investment in community-based teaching facilities and partnerships is critical for expanding experiential learning opportunities (Students learning medicine in general, 2016).
c. Student Services: Offer comprehensive support, including academic counselling, health and well-being services, and recreational facilities. Ensure an appropriate staff-student ratio (Malaysian Medical Council, 2020), and consistent quality assurance in community-based education (CBE) is also vital (Lee et al., 2014).
Discussion
While there are recent reviews in medical education (e.g. on curriculum evaluation frameworks, clinical reasoning curricula, competency-based education, AI in curricula, and research skills), none offer a broad comparison of different curriculum models across the field to the best of our knowledge. Most existing reviews specialise in a single domain or method, leaving a gap for a comprehensive, cross-model synthesis.
This review explored existing models of undergraduate general practice curriculum design and identified key principles guiding effective undergraduate medical education in this field. A key finding is the necessity of aligning general practice curricula with both universal competencies such as those outlined by frameworks like CanMEDS, RACGP, and RCGP and region-specific healthcare needs. These competencies provide a shared foundation for curriculum development, ensuring that graduates are equipped to deliver the broad scope of care required in family medicine.
This review examined how current curriculum structures addressing the early stages of curriculum design particularly, problem identification and general needs assessment align with Thomas et al.'s six-step model, a conceptual framework for curriculum development and Updation (Knowles, 1980; Thomas et al., 2015). These foundational stages are essential for identifying education gaps in the context of shifting population needs, evolving healthcare delivery models, and expanding expectations of GPs. Despite the widespread inclusion of core elements such as communication, continuity of care, and community orientation, substantial regional variability in delivery and emphasis persists (Raffing et al., 2023). For example, urban curricula may emphasise specialised care, while rural programmes prioritise continuity, generalism, and community involvement. These differences can influence graduate preparedness, with graduates from rural training programmes more likely to enter primary care residencies and practice in rural areas (Wendling et al., 2020).
A significant challenge highlighted in the literature is the shortage of clinical placement opportunities, particularly within family medicine clerkships. Evidence suggests that more than 80% of medical schools in the United States experience difficulties in securing adequate clinical sites and qualified instructors, a challenge likewise reported in Canada and the United Kingdom (Theobald et al., 2022). This shortage presents a barrier to comprehensive general practice education, underscoring the need for innovative solutions such as telehealth, simulation, and expanded community partnerships.
Additionally, the underrepresentation of vulnerable and marginalised populations in general practice curricula remains a critical issue. The healthcare needs of homeless individuals, asylum seekers, and other underserved groups are often insufficiently explored in education and training, despite the central role GPs play in delivering care to these populations. Addressing this gap is vital for producing well-rounded graduates who are equipped to serve all communities.
Finally, the concept of generalism, which emphasises a broad foundation of medical knowledge and skills, was found to be both vital and inconsistently supported across institutions. While some medical schools actively promote generalist principles, others lack the structural support or leadership necessary to embed these principles into their curricula effectively. Generalism should be a cornerstone of general practice education, supporting not only the individual GP's comprehensive knowledge but also interdisciplinary collaboration and continuity of care across health systems (College of Family Physicians of Canada, 2020).
These findings highlight the importance of developing curriculum frameworks that are adaptable, evidence-informed, and regionally responsive. Practical training, equitable care, and responsiveness to evolving healthcare priorities must remain central. This aligns with the recommendations of Parekh et al. (2021) who emphasised increasing the visibility of GP role models in clinical teaching and leadership, designing clerkships that offer meaningful, active participation and enabling students to experience the complexity, uncertainty, and real-world risk management inherent in general practice (Parekh et al., 2021).
These findings arrive at a critical juncture for Irish medical education. Undergraduate medical schools in Ireland are actively reviewing and restructuring their curricula, some with explicit aims to expand and strengthen General Practice teaching. This national momentum creates an opportunity to incorporate the global best practices identified in this review particularly around early exposure, longitudinal placements, interprofessional learning, and engagement with underserved communities into the next generation of Irish general practice education frameworks.
Methodological considerations
This review provides a timely synthesis of diverse literature across multiple countries, highlighting both shared priorities and emerging areas for undergraduate general practice curricula. As this is not a systematic review, a formal risk of bias assessment for study quality was not conducted. Though grey literature sources, including curricula and reports from national bodies (e.g. Medical Council of New Zealand, RACGP in Australia, Irish College of General Practitioners) and international organisations (e.g. WONCA), were included where available, it is possible that some relevant material was missed. Given the dynamic and contextual nature of medical education, the applicability of the themes identified in this review may change as curricula continue to adapt to shifting healthcare needs. Furthermore, significant variation in the structure, length, and quality of clinical placements across institutions means that these findings may not capture the full breadth of current practice.
Implications for practice and policy
Medical educators should advocate early and sustained exposure to general practice settings, with structured mentorship and integration of reflective practice. Interprofessional education and community engagement should be embedded into teaching strategies to address the diverse roles GPs play in modern health systems. Faculty development initiatives are essential to equip educators with the tools to deliver holistic, patient- and population-centred education. Educators can play a pivotal role in addressing gaps in representation by incorporating modules on marginalised populations and climate health into teaching content. Addressing the shortage of clerkship sites requires multifaceted solutions, such as developing new training sites, expanding search areas, utilising simulation and telehealth technologies, and offering incentives like Continuing Medical Education (CME) credits for teaching preparation (Association of American Medical Collegesb). A key element in linking clerkship sites to practices is understanding the unique demands of clerkship providers and incorporating these into the curriculum, thus facilitating better clinical placements and outcomes. Additionally, studies have emphasised the need for medical professionals to develop specialised skills to address the healthcare needs of vulnerable populations, such as the homeless in New York (Asgary et al., 2016) and asylum seekers in the UK (Kwok and Jacob, 2024). These findings reinforce the need for curricula to evolve to prepare students for these specific challenges.
Conclusion
This narrative review underscores the importance of designing undergraduate general practice curricula that are dynamic, community-responsive, and aligned with global best practices. While competency-based frameworks provide a shared foundation, clinical educators must tailor their approaches to reflect local health challenges, workforce demands, and educational resources. Prioritising practical exposure, interprofessional learning, and inclusion of underserved health themes will help shape graduates capable of meeting real-world primary care demands.
We would like to acknowledge support from University College Dublin's (UCD) School of Medicine and College of Health and Agricultural Sciences. Additionally, we extend our gratitude for the funding support provided to study investigators received through the UCD Clinical Research Centre and the Health Research Board.