This practice forum paper aims to present a theoretical framework to better develop the required supply chain management (SCM) competencies and the workforce needed for managing public health supply chains.
This framework is driven by iterative systems thinking, a deeper consideration of the SCM labor market and a comprehensive mapping of human resource system requirements. The framework centers around three tools. A labor market analysis assesses factors influencing supply of and demand for health SCM workers in a country context. To improve supply of and demand for workers, the SCM Professionalisation Framework provides reference documents to establish health SCM as a recognized profession. The human resources for SCM Theory of Change explains and assesses the conditions required to achieve optimal workforce performance at the organizational level. The Ministry of Health in Rwanda applied these three tools sequentially to assess and improve the supply and performance of its health SCM workforce.
The authors describe this framework, how the tools were applied in Rwanda, and early impressions of the results.
Practitioners can apply this approach to improve SCM competence and promote the attractiveness of health SCM positions by formalizing their professional status. This could lead to a pool of individuals who seek SCM qualifications and, in time, overcome the current shortage of health SCM workers. Employers can apply this approach to structured roles and workforce needs to meet health SCM system requirements. This would lead to a greater demand for and use of appropriately trained personnel.
This paper presents a novel, iterative, systems-thinking approach to develop human resources in public health supply chains. Rwanda is the first country to apply all three tools using this framework.
List of Abbreviations
- ADDIE
= Analysis, diagnosis, intervention development, implementation and evaluation;
- GHSC-PSM
= Global Health Supply Chain Program-Procurement and Supply Management;
- HSCM
= Health supply chain management;
- HR
= Human resources;
- HR4SCM
= Human resources for supply chain management;
- HRH
= Human resources for health;
- JD
= Job description;
- MOH
= Ministry of Health;
- PCC
= People that Deliver (PtD) Competency Compendium for Health Supply Chain Management;
- PtD
= People that Deliver;
- RMS
= Rwanda Medical Supplies Ltd;
- SAQA
= South African Qualifications Authority;
- SAPICS
= (the professional body for SCM in South Africa);
- SCM
= Supply chain management;
- TOC
= Theory of change;
- UHC
= Universal health care;
- USAID
= United States Agency for International Development; and
- WHO
= World Health Organization.
1. Introduction
The supply chain management (SCM) workforce responsible for health products plays a vital role in ensuring strong health systems exist. This workforce manages product selection, forecasting, procurement, storage, distribution and use of health commodities and incorporates pharmacists, supply chain managers, data managers, warehouse and transport personnel, among others (Seifman et al., 2013; Brown et al., 2019). Effective health supply chain management (HSCM) is a critical enabler for achieving universal health coverage (UHC), where all patients can access quality health services and affordable medicines without facing financial adversity (United Nations, 2015). Affordable medicines cannot be available to meet increased service coverage required by UHC without the reliable, cost-effective supply of quality medicines (Steele et al., 2022).
Managing the supply chain system effectively requires an adequate pool of qualified, competent workers (Chandani et al., 2014); yet, in many countries, an insufficient number of workers with required capacities exists (Dowling, 2011; Privett and Gonsalvez, 2014; Steele, 2014; Itiola and Agu, 2018; Lugada et al., 2022; Mekonnen et al., 2023). In many contexts, the workers responsible for HSCM are not given sufficient pre-service or in-service training for the SCM competencies required (Steele, 2014; Kasonde and Steele, 2017; Chukwu et al., 2017; Lugada et al., 2022). A review of literature related to HSCM workers in developing countries identified weaknesses in the skills required to:
quantify health product needs;
appropriately order, receive and store products; and
record inventories accurately (Brossette et al., 2010).
A literature review of the health supply chain in Uganda identified several additional workforce challenges, including vacancies in supply chain positions ranging from 10% to 55%, and other issues, such as insufficient supervision and workload, which could negatively impact workforce motivation (Lugada et al., 2022). In various contexts, issues surrounding human resources (HR) have been linked to poor supply chain performance (Dowling, 2011; Project Optimize, 2011; Sporrong et al., 2016; Kasonde and Steele, 2017), including stockouts (Mukasa et al., 2017; Olaniran et al., 2022).
A skilled workforce is a major factor in supply chain performance (Chandani et al., 2014); however, the skills and performance of SCM workers are often overlooked (McKinnon et al., 2017). Too often, HSCM workers are poorly recognized, and the supply chain is not valued as a critical support function of the larger health system (Brossette et al., 2010). In most contexts, the logistics sector suffers from low status of logistics workers and low prestige (McKinnon et al., 2017). In HSCM specifically, very often clinical staff, such as nurses or pharmacists, are tasked with SCM functions as an additional duty and SCM tasks are not clearly described in job descriptions (Meier et al., 2023). For example, in Uganda, fewer than 10% of health facilities had integrated SCM functions, such as ordering and reporting, under the responsibilities of pharmacy and store staff (Lugada et al., 2022). Although formal systems exist to train and professionalize clinical staff, formal systems often do not exist to professionalize HSCM staff and cultivate SCM skills. There is often no career path or professional organization for HSCM workers (Meier et al., 2023).
1.1 Problem statement
Current capacity development approaches for the HSCM workforce have only partially addressed the full range of issues in developing an adequate, appropriately skilled, motivated HSCM workforce. Labor market analyses are needed, along with a SCM professionalization process that considers the policies, regulations and national education requirements for HSCM professions. Historical approaches have not adequately addressed these elements and have not considered factors in the broader labor market. At the national level, there is a need for a broader perspective that:
looks beyond the existing individual and organizational workforce within the public health supply chain system;
considers the national labor market for HSCM workers in both the public and private sector; and
considers the educational competencies, regulations and accreditations influencing SCM workers.
At the organizational level, there is a need to define a comprehensive, explicit theory of change model expressing all components required for optimal HSCM workforce performance and to map how the components relate to one another and lead to improved supply chain performance.
1.2 Purpose
This paper presents a theoretical framework that enables practitioners to better develop the required SCM competencies and to manage the workforce required for optimizing public health supply chain performance.
1.3 Contributions
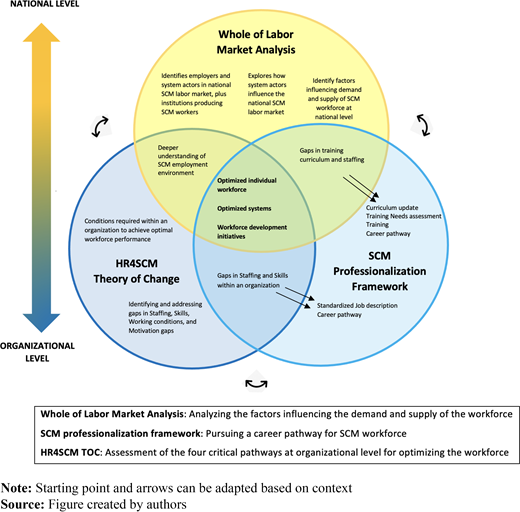
Our paper makes multiple contributions to the SCM workforce literature. First, we propose a theoretical model (see Figure 1) that explains the relationship between three critical tools that can be used together as a holistic approach to enable practitioners to improve the capacity and availability of human resources for SCM at the national, organizational and individual levels. The HSCM workforce literature has not described frameworks that simultaneously address workforce issues across these three levels or that specifically address the labor market for the HSCM workforce. Next, our model includes a theory of change that describes all conditions needed within an organization for optimized HSCM workforce performance and explains how workforce development activities link to this model. This is noteworthy as very few health worker capacity development interventions in the literature specify their theoretical foundations (Bergeron et al., 2017).
The paper is structured as follows: Section 2 discusses existing frameworks for developing the HSCM workforce, gaps in existing models and use of systems thinking in HR development. Section 3 presents the methodology used to develop this approach and implement this case study. Section 4 discusses the advantages, disadvantages, benefits and challenges of adopting this approach. Finally, Section 5 concludes the case study and suggests further research opportunities.
2. Literature review of existing frameworks
Historically, capacity development for the HSCM workforce has focused on improving the individual level, ranging from training individuals on SCM or leadership, to improving supervision (Gerdes and Pamela Steele Associates, 2016). Capacity development has also occurred at the organizational level, through activities to strengthen organizations, like ministries of health (e.g. through developing SCM strategies, creating committees to oversee the supply chain or implementing systems to capture SCM data) (Gerdes and Pamela Steele Associates, 2016). A limited focus has occurred on the national level (e.g. through initiatives to address policies on education curriculum or professional designations of SCM cadres).
Frameworks have been developed to address aspects of health workforce development (Seifman et al., 2013; USAID | DELIVER Project, 2013a; People that Deliver, 2014). For example, the Human Resource for Health (HRH) Action Framework, a general framework supporting governments to develop an effective health workforce, was applied to the HSCM workforce (Seifman et al., 2013; Global Health Workforce Alliance, 2024). The framework aimed to address issues, such as staff shortages, gaps in skills and competencies, low retention and poor motivation. The HRH Action Framework defined “HR Management Systems” as one of its six action areas. To improve “HR Management Systems”, the framework outlined three necessary areas: HRH information, workforce planning and performance management and retention. Under this framework, improved collection of HRH information could be used to develop workforce policies (e.g. on performance management and retention), along with education strategies, to ultimately improve the supply chain workforce (Seifman et al., 2013). The HRH Action Framework defined a linear action cycle: “Situational Analysis”, “Planning”, “Implementation”, “Monitoring and Evaluation”, which promoted conducting an HR situational analysis and applying the results to generate and implement workforce plans, and then monitoring and evaluating implemented activities (Seifman et al., 2013).
In addition, USAID adapted the CapacityPlus Framework (USAID | DELIVER Project, 2013a) to guide HR initiatives in its HSCM projects. The framework describes five foundational components to develop HR. These components are:
“Build powerful constituencies” (i.e. stakeholders who provide technical leadership in SCM and HR);
“Optimize policies and plans” (that support “HR capacity development”);
“Develop workforce” (i.e. activities “including recruiting, competency modeling and development, and pre-service and in-service education”);
“Increase workforce effectiveness or performance management” (i.e. activities such as retention, supervision and mentoring); and
“Professionalization of SCM” (i.e. the process to establish SCM roles as a profession) (USAID | DELIVER Project, 2013a).
The CapacityPlus Framework provides a high-level summary of the ideal elements needed within a country’s HR system for HSCM; however, the framework does “not directly tie the benefits of high performance within these areas to improved commodity availability” or improved workforce performance (Gerdes and Pamela Steele Associates, 2016). The framework did not explicitly explain how interventions to improve the five foundational components could link to one another or how such interventions could improve workforce performance.
Standardized assessment tools (USAID | DELIVER Project, 2013a; Remmelzwaal and Kasonde, 2016) have been developed to identify specific HR problems at the organizational or individual levels, and constructive, sound resources (People that Deliver, 2014) have been prescribed to address the problems the assessment tools revealed. For example, the USAID HR Capacity Development in Public HSCM: Assessment Guide and Tool (USAID | DELIVER Project, 2013a) was applied in various contexts to complete a rapid, comprehensive assessment of the HR system supporting a country’s supply chain. These assessments enabled linear, stepwise methods to diagnose and remedy issues, such as weak annual performance management processes, high staff turnover, decreasing budget for salaries or insufficient training opportunities (People that Deliver, 2014). Suitable interventions occurred, focused on appropriate activities at the individual and organizational levels, such as recruiting quality employees, conducting training, developing employees through SCM competency modeling, retaining employees and increasing workforce productivity (USAID | DELIVER Project, 2013a).
2.1 Gap analysis
A 2016 assessment of prior interventions in HR for HSCM across multiple years identified that interventions were applied in a standalone approach and were typically reactive, driven by issues revealed through assessments; however, a proactive theory of change explaining the logical foundation of interventions and how interventions led to improved SCM, or workforce performance was lacking (Gerdes and Pamela Steele Associates, 2016). This gap made it difficult to assess the interventions’ levels of success. Meanwhile, concerns grew that HR development through training alone was neither sufficient nor sustainable. A review of interventions to improve HR in the health space found that “increased knowledge and skills through training was an important mechanism to contribute to improved performance, but not sufficient” (Dieleman et al., 2009). At the same time, the view grew that a traditional, transactional approach to HR development through conducting ad hoc trainings would not be cost-effective nor sustainable over the long-term, as these events required continuous external support (USAID | DELIVER Project, 2013b). Despite investments needed in other areas, staffing and training remained a major focus of workforce development approaches. A business case study of donors’ budgeted investments for SCM HR at a country level revealed that significant investments were made in staffing (usually through salaries) and training SCM staff; however, broader workforce issues and enablers, including motivation and working conditions, had been neglected (People that Deliver, 2023). Similarly, an analysis looking at activities to improve HR in the health field across three international agencies found that short-term, in-service training was by far the most common activity, with little investment in pre-service training capacity (Vujicic et al., 2012).
The literature suggests additional potential shortcomings of historical approaches. Individual- and organizational-level approaches typically follow a linear process of analysis, diagnosis, intervention development, implementation, and evaluation (ADDIE), which Bierema and Eraut (2004) argue could be limited in addressing organization complexity and power dynamics. Workforce development navigates complex environments and systems. Despite this, very often, HR development views these systems as complex linear systems, rather than “nonlinear dynamic, interdependent systems” (Yawson, 2013). Bierema and Eraut (2004) suggest that HR development instead “should ideally be implemented with a systems and long-term focus”.
Although prior SCM HR approaches involved several formulas for addressing individual- and organizational-level change (e.g. ADDIE, performance improvement, training), the SCM workforce development space has not applied a broad, systems approach. Despite how the SCM labor market strongly influences the availability and use of SCM workers, the sector has not addressed how SCM HR development interacts with the wider labor market system. Very few initiatives have addressed the higher-level systems and national policies impacting the education, regulation and development of workers to improve the availability and skills of this workforce. McKinnon et al. (2017) argue that SCM workforce development depends not only on organizational HR policies; it also requires national initiatives to educate for SCM occupations. Beyond companies and their employees, other stakeholders such as logistics associations, higher educational institutes and vocational training institutions have a mutual interest in the education, training and development of logistics employees, individually and collectively (McKinnon et al., 2017).
At the same time, a theory of change model that provided a theoretical explanation to 1) explain how standalone individual and organizational interventions connected to one another, 2) describe how these activities connected to the ideal SCM HR system and 3) explicitly state how these activities ultimately improved supply chain performance, was lacking (Gerdes and Pamela Steele Associates, 2016). A systematic review of capacity building in the health sector found this lack of theoretical framework to be widespread. A limited number of published capacity building interventions specified their theoretical foundation, and those interventions that did explicitly identify a specific framework, model or theory typically did not explain how those concepts were applied (Bergeron et al., 2017). “Assumptions underlying HR management interventions are usually not made explicit, hampering our understanding of how HR management interventions work” (Dieleman et al., 2009).
2.2 Systems thinking approach to workforce development
Systems theory is a foundational theory of HR development; however, gaps exist between reference to this theory as a foundation and applications of systems thinking in practice (Yawson, 2013). Systems thinking is a structured thought process that considers the interrelationships between the parts of a system and how subsystems work within a larger system (Rosas, 2017). Systems thinking aims to see “how things are connected to each other within some notion of a whole entity” and to reveal and express the common principles governing the system (Peters, 2014). This process helps to systematically identify the causes of a problem from a non-linear perspective and to find solutions; it is particularly useful in understanding change that is not linear (Rosas, 2017).
The HR system supporting HSCM in a country is a complex, interdependent system, involving elements operating on the individual-, organizational- and national-levels that develop and change in non-linear ways. HSCM workers are employed within an organization. They may also have a connection to a training institution or professional association. In addition, the HSCM workforce is part of a broader labor market system, where they are part of the supply of workers. This workforce and labor market also operate within the larger enabling environment of professional, educational and accreditation regulations. This legislative and policy framework at the national level involves the organizations that employ SCM workers and the education institutions that supply SCM workers (Meier et al., 2023). Modifying higher-level legislative and policy frameworks at the national level can impact the supply of and demand for SCM workers.
Systems thinking involves bringing together interdependent systems to work in a coordinated process toward common goals (Peters, 2014). This paper presents a series of tools that enables practitioners to better describe and improve the development of human resources for SCM by comprehensively addressing the interdependent parts of the SCM HR system. The Human Resources for SCM Theory of Change (HR4SCM TOC) (Supplementary File 1 and Supplementary File 2) is an explicit model that defines 60 organizational-level requirements for the HR system supporting SCM. The SCM labor market analysis conceptualizes how the organizational-level HR system interacts with and is part of a larger system: the national-level labor market for SCM workers and identifies issues in the labor market. The SCM Professionalisation Framework provides reference documents and a detailed implementation approach (Supplementary Files 3–7) for countries to establish HSCM as a recognized profession at the national level.
3. Methodology
3.1 Development of the tools
3.1.1 Development of the human resource for supply chain management theory of change
In 2016, USAID engaged consultants to conduct a retrospective analysis of USAID’s investments in HR4SCM, over multiple years, and to ascertain the level of success of prior interventions (Gerdes and Pamela Steele Associates, 2016). The report acknowledged that prior interventions had not been designed with an eye toward evaluating impact. Specifically, a pathway to connect whether the interventions were contributing to a higher-level objective, such as increasing supply chain performance overall, was lacking. This deficiency could be rectified with a theory of change (TOC) for maintaining an optimal HSCM workforce. The report contained an early draft of a TOC model (Gerdes and Pamela Steele Associates, 2016).
An interactive workshop in Tanzania engaged 54 public health supply chain stakeholders, ranging from academics to practitioners, to provide feedback on the initial TOC. Seven moderators facilitated small group discussions and captured notes. The main findings indicated the proposed TOC was both an oversimplification and had a level of complexity that prevented it from being used as a stand-alone framework.
From this starting point, People that Deliver (PtD) [1] engaged experts in TOC methodology to further develop a TOC model for building an optimal HSCM workforce. In collaboration with PtD, external experts clarified the long-term outcome, refined outcome pathways and added underlying rationales, along with potential interventions and indicators for each outcome. PtD leaders provided feedback on the outcomes map in several recorded meetings to finalize the HR4SCM TOC model (Supplementary File 1 and Supplementary File 2).
During the refinement process, stakeholders identified that this TOC focused on optimizing productivity at the organizational level. Although the TOC highlighted the need for multiple policies, this tool did not include concepts around labor market analyses, an approach the World Health Organization (WHO) was promoting for clinical health cadres at that time. Further, the TOC did not provide specific guidance on how to professionalize the HSCM workforce.
3.1.2 Development of a supply chain management labor market analysis approach
PtD developed a labor market study methodology that used qualitative approaches to capture factors affecting supply and demand of the HSCM workforce in Rwanda. The methodology sought to obtain employer and employee perspectives about practices that affect supply and demand of SCM labor, while also exploring tacit knowledge about the broader SCM labor market. The methodology was informed by work from the WHO on health labor market analyses (Scheffler et al., 2012; Sousa et al., 2013; WHO, 2021) and was designed to generate:
a detailed understanding of the stakeholders in the SCM environment;
a descriptive overview of the supply and demand factors influencing the availability of SCM professionals; and
a profile of the SCM employment landscape in a country context.
3.1.3 Development of a supply chain management professionalization framework
First, PtD conducted semi-structured interviews with 10 leading SCM organizations to explore perspectives on how to create a framework for professionalizing the HSCM workforce. Interview data was analyzed using direct thematic analysis and findings were validated through a validation workshop (Brown et al., 2024). Next, PtD developed the first component of its SCM Professionalisation Framework: The Library of Competencies and Designations (Supplementary File 3 and Supplementary File 4). This is a competency framework with a detailed description of HSCM competency requirements across job maturity levels. PtD reviewed existing competency frameworks from the public and private SCM sectors to compare content and structure (Brown et al., 2024). Two frameworks were selected as primary frameworks to inform the SCM Professionalisation Framework:
People that Deliver (PtD) Competency Compendium for Health Supply Chain Management (PCC) (People that Deliver, 2014); and
the Supply Chain Competency Framework from SAPICS, the professional body for SCM in South Africa.
The PCC defines all competencies needed within a national health supply chain. The Supply Chain Competency Framework from SAPICS describes SCM competencies in 11 competency areas and defines a career progression with five designation levels.
PtD selected the PCC to serve as the basis for the HSCM competency framework and compared the PCC against the SAPICS framework to validate content and the structure of the competency framework (Brown et al., 2024). PtD reviewed public and private sector SCM job descriptions and hierarchical structures to create professional levels. Across reviewed materials, PtD identified that five professional designations (or levels) would be the ideal structure: Associate, Practitioner, Specialist, Professional and Leader. Bloom’s Taxonomy of Educational Objectives (Armstrong, 2010) was applied to define increasing levels of expertise across the five levels (Brown et al., 2024). With five professional levels defined, PtD specified the behavioral competencies needed across the five professional levels for each competency in the PCC.
Next, PtD developed the second component of its professionalization framework: The Mapping of Education (Supplementary File 6), which is a listing of qualifications and available educational offerings for each behavioral competency and designation level. To list qualifications and available courses, PtD selected the South African Qualifications Authority (SAQA) as an example of a national education framework to use as a foundation. This registry catalogs all education programs in South Africa. First, any qualifications not related to domains in the Library of Competencies were removed. Next, using natural language processing algorithms, PtD compared its behavioral competencies with SAQA course descriptions, identified matches and included these matches in the Mapping of Education (Brown et al., 2024). Finally, additional education sources were reviewed for relevant courses, such as the Association for SCM and Chartered Institute of Procurement and Supply, among others (Brown et al., 2024).
Thereafter, PtD created the third framework component: the Collection of Roles and Job Descriptions for Health Supply Chains (Supplementary File 5), which is a reference guide of sample job descriptions. Using this guide, SCM employers can translate the framework’s behavioral competencies into job descriptions. PtD used its previously developed job description (JD) catalog (Federal Ministry of Health Sudan, 2017) as a basis for this guide. PtD reviewed this JD catalog and sample organizational hierarchies to identify and define hierarchical levels for common roles within an organization. Four levels were defined: strategic, managerial, operational and tactical. These aligned to the competencies and designation levels in the Library of Competencies and Designations. PtD assigned a professional designation level for each sample JD and drew from the Library of Competencies and Designations to assign the relevant competencies and behavioral competencies for each position. Next, PtD drew from the Mapping of Education component to state potential education requirements for each JD and added sample key performance indicators (Brown et al., 2024).
Finally, PtD developed an Implementation Approach (Supplementary File 7) to give countries a unified methodology for applying the components of the SCM Professionalisation Framework. PtD defined five steps for the Implementation Approach, based on the optimal way to apply the framework components and logical sequencing, then defined deliverables and key objectives for each step.
3.2 The tools
In developing this approach, concepts from system thinking were applied to ensure the resulting approach addressed all parts of the HSCM HR system. Overall, PtD adopted a systems perspective that viewed the HSCM workforce as part of and affected by multiple, interacting subsystems (Hargreaves, 2010). PtD then considered the “boundaries, relationships, and perspectives” of these subsystems (Midgley, 2007). HSCM workers are part of organizations employing them. The HR4SCM TOC defines the organizational-level requirements for these organizations. After mapping the organizational requirements, PtD targeted the labor market system that impacts whether there is an adequate pool of skilled workers for organizations to recruit. The labor market analysis approach identifies actors in the labor market system through network mapping and then gathers perspectives of these actors on factors influencing supply and demand of workers. The SCM Professionalisation Framework further engages this diverse network of stakeholders and provides stepwise guidance to establish HSCM as a profession at national level. As PtD reflected on the iterative process to create these three tools, PtD developed a model to show how the tools interrelate and to describe expected outcomes across the national, organizational and individual levels. Figure 1 summarizes this model.
3.2.1 Labor market analysis
A country’s HR system supporting SCM interacts with a broader system: the national SCM labor market. Considering the supply of and demand for SCM labor in a country context, along with the national legislation and policies that drive how the labor market operates, provides a deeper understanding of the SCM employment environment. These labor market insights are needed to fully realize adequate staffing and appropriate skills. By conducting a SCM labor market analysis, countries can understand 1) issues in the availability of SCM human resources, 2) issues in the demand for or use of the SCM workforce, 3) skill gaps and 4) how certain policies may be restricting the labor market. Critically, the analysis also maps the stakeholders in the SCM labor market, including government ministries, professional bodies, private sector SCM or pharmaceutical companies and educational institutions producing SCM workers.
Once issues in the labor market have been identified, policies can be developed to shape the labor market to ensure the career path, education opportunities and professional growth for SCM workers are aligned with demand for workers. This alignment in supply of and demand for workers will ultimately grow the pool of appropriately skilled workers. Are there factors around how the SCM profession is defined, regulated and organized contributing to market imbalances? On the demand side, are organizations asking for the right cadres and competencies? Are these organizations offering appropriate remuneration and working conditions to draw talent? On the supply side, do SCM workers demonstrate adequate technical competencies suitable for the local context? What types of education opportunities are needed to fill identified skill gaps? Are educational establishments producing workers with the required qualifications and skills? What factors influence how HSCM workers move across organizations? Once a labor market analysis answers these questions, adopting the PtD SCM Professionalisation Framework (Supplementary Files 3–7) can facilitate a coordinated process to address these issues, while engaging a broad coalition of stakeholders, and to ultimately catalyze the labor market for the benefit of all SCM sectors (dos Santos et al., 2020).
3.2.2 People that Deliver supply chain management professionalisation framework
Building off an improved understanding of the labor market, the SCM Professionalisation Framework (Supplementary Files 3–7) provides a methodology to engage all stakeholders with a view to catalyze the labor market, improving the availability and use of SCM workforce. The SCM Professionalisation Framework defines SCM competencies by level and provides a list of educational opportunities to achieve competencies. Governments and organizations can build upon this information to explicitly state SCM competency requirements, education requirements and a career path. Adopting a SCM professionalization framework can ultimately seed the employment environment with a sustainable pool of workers and generate demand for this workforce by employers.
The SCM Professionalisation Framework can be applied in any country context to improve the availability and use of HSCM professionals. It provides the guidance needed to create a skilled workforce in the private and public sectors and to improve SCM outcomes. As described earlier, it centers on four resources:
the Library of Competencies and Designations (Supplementary File 4);
the Collection of Roles and Job Descriptions for Health Supply Chains (Supplementary File 5);
the Mapping of Education (Supplementary File 6); and
the Implementation Approach (Supplementary File 7), which provides guidance on how to work toward professionalization of this workforce.
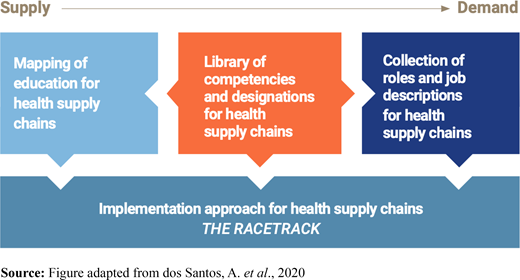
Figure 2 shows how the four components of the PtD SCM Professionalisation Framework fit together. The core component is the Library of Competencies and Designations (Supplementary File 4), which supports standardization of all competencies and designations needed within a national health supply chain. It presents seven competency domains that cover the practice of HSCM across the public and private sectors (Selection & Quantification; Procurement; Storage, Use & Dispense; Resource Management; Professional; Personal; and Technology) and provides “behavior statements” outlining workplace expectations in all listed competency domains. It also provides a five-level designation classification for each competency area from Associate to Leader. Definitions for the five professional designations are listed in Table 1.
On the demand side, the Collection of Roles and Job Descriptions (Supplementary File 5) answers what competencies are required for a particular job role, referencing the competencies in the central component, the Library of Competencies and Designations. The collection provides a systematic way to build job descriptions and enables employers to create demand for skilled SCM practitioners. It is also a starting point for organizations that need to confirm that they possess all necessary competencies across their workforce. It includes sample organizational charts, job descriptions and key performance indicators.
On the supply side, the Mapping of Education (Supplementary File 6) shows how education and training align to job roles and lists what courses are available to develop each specific competency. It includes more than 250 courses from various providers around the world. The Mapping of Education gives the user a broad idea of the types of education that are available to fill in the skills gaps found in a country, recognizing that each country may have its own regulations and prerequisites.
Finally, the Implementation Approach for Health Supply Chains (Supplementary File 7) provides countries with a standardized process to adopt the PtD SCM Professionalisation Framework to align career path, education and professional growth in HSCM. This process encompasses national and organizational actions. Overall, adopting the PtD SCM Professionalisation Framework can enable:
governments to define SCM professional standards and competencies;
employers to set their desired SCM competency requirements when developing SCM job descriptions;
educational institutions producing SCM professionals to align curricula to standards and needs; and
the SCM workforce to chart their career path (dos Santos et al., 2020).
3.2.3 Human resources for supply chain management theory of change
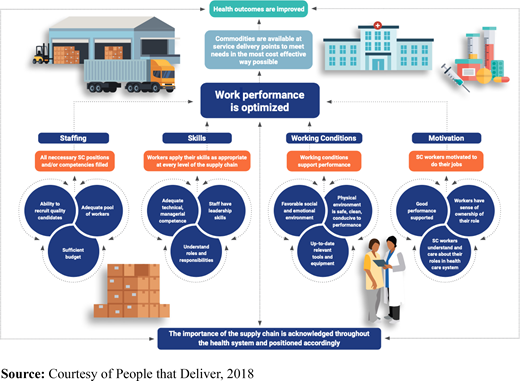
The PtD Human Resources for Supply Chain Management Theory of Change (HR4SCM TOC) explains how PtD’s systems thinking approach conceptualizes the HR system supporting SCM at the organizational level (e.g. ministries of health, national supply chain organizations). The framework explains the 60 conditions that must exist in an organization’s HR system supporting HSCM to optimize workforce performance. (Full diagram of the 60 conditions is available in Supplementary File 2). Required components build on one another in a chain of results and are organized in four distinct causal pathways: Staffing, Skills, Motivation and Working Conditions. This comprehensive mapping of requirements enables stakeholders to acknowledge and articulate a common understanding of the essential components of the HR4SCM system.
Through a diagnostic exercise using this theory of change, HSCM stakeholders can compare the country’s existing HR system against the required components of the HR4SCM TOC and identify which elements are missing at the organizational level (Brown et al., 2019). The HR4SCM TOC can then provide a prospective, theory-driven process to design workforce interventions that build required components. For instance, targeted interventions are well-suited to develop the required conditions in the Working Conditions pathway. Introducing policies that support a favorable organizational culture, creating an occupational health and safety system or providing workers with needed equipment are examples of activities that can be accomplished through discrete, time-limited interventions to develop key conditions in the Working Conditions pathway (Steele et al., 2020).
On the other hand, complex, broad and system-wide coordination is needed to develop the highest-level conditions of the Staffing and Skills pathways. The highest-level conditions of the four causal pathways are shown in Figure 3, a simplified version of the HR4SCM TOC. (The full outcomes map is shown in Supplementary File 2). Ensuring that an “adequate pool of workers exists” and that “employers can recruit quality candidates” –two of three top conditions of the Staffing Pathway– and that “adequate technical, managerial competence” exists in the Skills pathway require looking at the labor market for HSCM workers and developing a SCM professionalization framework to define SCM professional standards and competencies, then aligning these standards with curricula.
3.3 Application in Rwanda
In Rwanda, public sector health facilities experience poor availability of medicines (Bizimana et al., 2020; Uwizeyimana et al., 2021) and limited capacity for SCM among the HSCM workforce, creating challenges at various system levels (Rwanda Ministry of Health, 2017; Kigenza et al., 2023). The Rwanda Ministry of Health (MOH) has deployed strategies to improve workforce capacity and motivation through approaches including supportive supervision, mentorship and continuous learning efforts (Rwanda Ministry of Health, 2014; Rwanda Ministry of Health, 2017).
Regulations in Rwanda require pharmacists to manage the health supply chain. Rwanda Medical Supply Limited (RMS Ltd) branches distribute pharmaceutical products to hospitals and health centers (Rwanda Ministry of Health, 2021; Uwizeyimana et al., 2021); at health centers, nurses typically manage SCM as an additional task (Meier et al., 2023). Although pharmacists are in place at each RMS Ltd branch, for many positions, the SCM tasks and functions are not defined, which are the basis for staff development, deployment and integration of clear SCM job descriptions (Meier et al., 2024). SCM competencies had not been formally mapped for all SCM services and assigned to SCM roles.
We applied the PtD systems thinking approach in Rwanda to improve HR development for HSCM workers. Table 2 describes the overarching methodological roadmap of how this approach was implemented in Rwanda. Although we applied the tools in a certain order in Rwanda, it might be more appropriate to start with a different tool and to apply the tools in a different order in other country contexts. We followed an iterative approach. In each phase, we identified the problem to be addressed, applied the appropriate tool, reflected on the results and discussed next steps with local stakeholders, based on findings. We then moved to the subsequent phase to address gaps in the next component of the system.
In October 2018, the MOH of Rwanda, with the support of USAID Global Health Supply Chain Program-Procurement and Supply Management (GHSC-PSM) project, conducted a study using the HR4SCM TOC to assess how Rwanda’s HR system for SCM compared to the 60 components in the HR4SCM TOC (Supplementary File 2). This study identified over 30 conditions required for optimal workforce performance that were missing in the Rwandan HR system and suggested interventions to build some of these missing components (Meier et al., 2024). Standalone interventions were developed to build components in the Motivation and Working Conditions pathways – such as creating a list of necessary tools and equipment for each level and requirements for a safe work environment (Meier et al., 2024). Missing components in the Staffing pathway – such as the ability to develop the right job descriptions or ensuring education is available for all required qualifications – called for a coordinated process with cross-cutting stakeholders to develop a professionalization framework for SCM in Rwanda (Meier et al., 2024). Table 3 lists the missing components in the Rwanda system that would be developed through the SCM professionalization process. Meanwhile, components of the Staffing and Skills pathways that required gathering more insights through a labor market analysis are listed in Table 4.
In March 2019, Rwanda’s MOH with support of the GHSC-PSM project completed a SCM labor market analysis, a qualitative study that gathered insights from government, professional associations, SCM employers and universities on factors affecting the pool of qualified SCM workers and organizations’ demand for workers. The analysis identified weak supply of, and demand for, the SCM workforce across a variety of industry sectors (Meier et al., 2023). On the supply side, the skills and competencies in the pool of SCM workers did not align with the needs of the employers. On the demand side, budget restrictions limited demand and employers had not clearly defined competencies the jobs required, nor the numbers of workers needed for workload (Meier et al., 2023).
Key factors contributed to gaps in the supply of skilled workers. An SCM career path and SCM professional standards did not exist (Meier et al., 2023; Meier et al., 2024). SCM curricula at the educational institutions producing workers did not match the needs of the labor market (Meier et al., 2023). Supply and demand factors would need to be coordinated to correct imbalances in the labor market, and a career path would need to be developed to encourage growth in number of SCM workers.
In 2020, the GHSC-PSM project led advocacy efforts to develop a framework to guide the professionalization of HSCM workers in Rwanda. The HR4SCM TOC and labor market analysis findings served as evidence of the existing gaps that a professionalization process would address. In 2021, a cross-cutting team began a phased process to create a SCM professionalization framework, guided by the Implementation Approach for Health Supply Chains (Supplementary File 7). Table 5 shows the various stakeholders engaged in the professionalization process, which would adapt the PtD SCM Professionalisation Framework to the local context.
In Rwanda, professionalization efforts are first aligning elements in the public sector, starting with Rwanda Medical Supplies Ltd (RMS) central store and its 30 regional branches, before expanding to the health facility level. The country will then focus on establishing a regulatory institution that will establish regulatory roles and potentially provide accreditation to the national regulatory board for supply chain professionals. The framework will also be applied in the education sector to establish training needs and gain support of the relevant educational institutions.
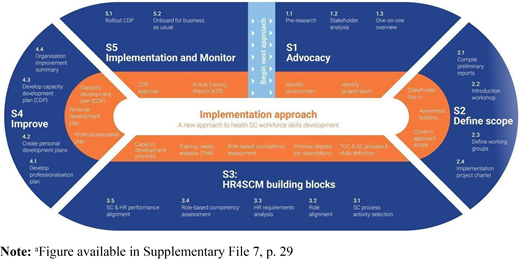
Figure 4 shows an overview of the SCM Professionalisation Framework Implementation Approach. In Step 1, Advocacy, the HR4SCM TOC study and results of the labor market analysis were used as pre-research to show the need for professionalization. The labor market study also included a stakeholder analysis that uncovered all public and private stakeholders involved in the SCM labor market. These stakeholders were then engaged in the professionalization process and the project team was identified.
In Step 2, Define Scope, the project team convened an introductory workshop with 42 participants from 16 stakeholder organizations. They defined working groups and developed a project charter and an overall project plan for implementing the framework components. The team is currently guiding stakeholders through Step 3, HR4SCM Building Blocks, which considers job roles and role alignment. So far, the application of the SCM Professionalization Framework and its process mapping tool has established standard SCM job descriptions for 4,083 staff across Rwanda Medical Supplies, Regional RMS, teaching, referral, regional and district hospitals and health centers in the public health sector. It also generated 607 learning objectives in 76 competency areas from 7 SCM domains.
4. Discussion
With a global focus on achieving Universal Health Coverage, there is a strong need to strengthen HR capacities at individual, organizational and national levels. In this paper, we have proposed a three-part, systematic approach that can be applied in any country context to improve the availability and use of SCM professionals for health supply chain operations. We hypothesize that professionalizing, resourcing and motivating the HSCM workforce, through the approach described in this paper, will lead to greater availability of workers and greater efficiency in workforce management. This is expected to lead to more satisfied workers, lower overall costs and improved performance.
A comprehensive, systematic approach is necessary to guide countries and practitioners to 1) consider all requirements at the organizational level for an optimized HSCM workforce, 2) investigate factors influencing the supply and demand of the SCM workforce at the national level and 3) develop a SCM professionalization framework to define SCM professional standards and competencies and align these standards with educational curricula. The literature has identified lingering concerns related to the short-term nature of activities to improve the health workforce and the viability of donor funding for creating sustainable health systems (Micah et al., 2022). A systematic review of approaches in the health sector to improve worker performance found that training or supervision alone typically had only moderate effects (Rowe et al., 2018). Another study argued that applying health labor market logic to policy and strategy approaches can help organizations to better understand the factors affecting workforce supply and demand at national levels, and ensure that strategies are comprehensive (Nove et al., 2023). Previous research in community health SCM has indicated that comprehensive approaches to workforce development can lead to improved data availability and product availability (Chandani et al., 2014).
On the demand side of the labor market, the World Bank has contended that organizations employing SCM workers must improve their HR policies and retention efforts by providing transparent career paths, optimal working conditions and investments in workforce development (McKinnon et al., 2017). Each of these factors is included in the HR4SCM TOC requirements and developed through the SCM Professionalisation Framework’s Implementation Approach. To improve the production and supply of SCM workers, the World Bank has highlighted that governments play a critical role in establishing regulation, enabling training or facilitating initiatives to ensure the available pool of workers has adequate SCM competence (McKinnon et al., 2017). Public interventions to improve SCM competencies could include:
supporting education and training at public institutions;
education policy and appropriateness of curricula; and
creating and harmonizing competency standards for SCM jobs.
The SCM Professionalisation Framework’s Implementation Approach facilitates the multi-stakeholder collaboration required to carry out these activities in a country context.
The HSCM workforce literature has not described other frameworks that address workforce issues simultaneously across individual, organizational, and national levels or that specifically address the labor market for the HSCM workforce. The Human Resource for Health (HRH) Action Framework is a general framework that supports governments to plan for and manage an effective health workforce; this framework was later applied to the development of the HSCM workforce (Seifman et al., 2013; Global Health Workforce Alliance, n.d.). Although this framework describes the general areas where actions can be planned to improve the HSCM workforce, this tool does not identify specific individual-level and organizational-level requirements. While the HRH Action Framework suggests considering the national labor market and recognizing HSCM professions, it does not provide specific guidance on how practitioners can assess market conditions or take defined actions to professionalize this workforce.
In sectors outside HSCM, frameworks and approaches to improve human resource capacity have tackled some of the elements addressed by the approach described in this paper. Pursuits to professionalize the workforces in other sectors, one element of this three-part framework, are in various stages of progress. For example, the humanitarian sector has pursued initiatives to professionalize some of the sector’s many professions (Walker and Russ, 2010; Walker et al., 2010; Bioforce, 2020) and has developed competency frameworks for certain humanitarian professions (Meeker et al., 2014; Core Humanitarian Standard Alliance, 2017; Vardanyan et al., 2018). Despite this progress, a study of humanitarian professions found that very few areas have succeeded in creating agreed competency frameworks or certification mechanisms for workers in these professions (Bioforce, 2020).
The literature around the humanitarian and commercial supply chain sectors includes calls for research into the connection between HR management and SCM performance; however, few frameworks describing how to connect the two topics exist. In the humanitarian supply chain sector, a 2022 literature review proposed a research agenda to investigate and verify how HR practices contribute to humanitarian supply chain performance (de Camargo Fiorini et al., 2022). In the commercial SCM sector, limited studies have moved beyond research agendas and have sought to demonstrate the implications of HR management on SCM (Alam and Syarifudin, 2018; Evangelista et al., 2023). Although some studies have described the connection between HR management practices and SCM (Gowen and Tallon, 2003; Shub and Stonebraker, 2009; Ellinger and Ellinger, 2014; Hohenstein et al., 2014; Gómez-Cedeño et al., 2015; Liboni et al., 2019), the literature lacks comprehensive frameworks detailing how to develop human resources in the commercial supply chain sector.
4.1 Potential advantages and disadvantages of the People that Deliver systems thinking approach
There are multiple advantages to the three-part HR development approach described in this paper. First, the model reveals the different entry points for assessing workforce issues and designing interventions to overcome workforce development challenges, along with very specific steps to implement solutions. Second, it provides an implementation framework with specific tasks to construct a reliable, holistic practice that considers how workforce development factors in a country are interconnected. Third, it guides government, donors and implementing partners in scoping workforce development projects in a country and determining investment priorities in a holistic manner.
In terms of disadvantages, adopting the systems thinking approach to workforce development in a country could threaten established processes and procedures. This could occur if, for example, resulting recommendations require major overhauls that might be resisted. Second, seeing gains from this approach requires considerable investment in all three intervention areas, using the prescribed tools, because challenges in one area may trigger ripple effects in other areas. Finally, adopting this approach could threaten social norms surrounding existing professional cadres. For example, pharmacists might feel threatened if some tasks previously assigned to this cadre are reallocated to a new professional role.
4.2 Benefits of adopting the People that Deliver systems thinking approach
Several potential benefits come from adopting this approach. The PtD systems thinking approach establishes methods that drive strategies, processes and procedures to align with the overall objectives for an ideal HR system for HSCM, which are defined in the HR4SCM TOC model. The approach provides a strategy based on a more comprehensive understanding of gaps in the required organizational-level factors, national-level labor market factors and national-level policies and actions needed to professionalize the SCM workforce. Interventions associated with this process are backed by the logic in the HR4SCM TOC. Explicitly stated logic is often lacking from capacity building interventions in the health sector (Dieleman et al., 2009; Bergeron et al., 2017).
The PtD systems thinking approach engages a broad coalition of stakeholders to pursue a cohesive, long-term improvement agenda focused on simultaneously improving multiple levels of the complex systems surrounding the HSCM workforce. Prior studies emphasize that HR development “should ideally be implemented with a systems and long-term focus” (Bierema and Eraut, 2004).
This approach provides standardized processes for applying similar tools and allows countries undertaking this approach to learn from one another. In addition, the PtD SCM Professionalisation Framework Implementation Approach standardizes the implementation process across countries, while the components of the SCM Professionalisation Framework enable a standardization of terms, framework structure and base-level standards for competencies. A better understanding of the applications, issues and successes at each phase of the Implementation Approach will help improve adoption in other countries. The HR4SCM TOC has been used as a diagnostic tool in Cameroon, Pakistan, Malawi, Democratic Republic of Congo, Thailand, Vietnam, Ukraine, Sierra Leone and Nepal. The SCM Professionalisation Framework is being adopted in Mozambique and Nigeria. Rwanda is the first context in which these two tools have been combined, along with the SCM labor market analysis, to apply the PtD systems thinking approach to health supply chain workforce development.
4.3 Challenges of adopting the People that Deliver systems thinking approach
A multi-year process planned in phases is needed to complete the application of this approach. Engaging stakeholders in a long-term improvement agenda to enhance a complex system brings challenges. The project team in Rwanda identified the following potential challenges to mitigate throughout this process:
engaging many stakeholders, while maintaining a common understanding and strong communication;
maintaining momentum during a long process;
working with limited budget and identifying financing to support the cooperative approach throughout the full process;
maintaining support of decision makers;
simultaneously engaging at the national level for structural and policy changes as well as at the organizational level;
managing resistance to change and change management;
ensuring proper rollout and implementation of the final SCM Professionalisation Framework; and
effectively communicating that it takes time to see impact following implementation.
4.4 Potential implications for practice
We propose a framework to encourage practitioners to move beyond a focus on HR development simply as training at the individual level and help practitioners to adopt systems-based approaches to improve the availability and use of SCM professionals. We believe that applying this framework has the potential to catalyze the national labor market to improve supply of and demand for HSCM workers. By moving from a limited focus on workforce training to comprehensively considering all elements influencing organizational and worker productivity, this approach has the potential to optimize systems, improve workforce development initiatives and optimize individual workforce performance. Assessing the labor market identifies key issues affecting the supply of and demand for skilled SCM workers so that imbalances can be remedied.
In the short term, the reference guides in the PtD SCM Professionalisation Framework can lead to several tangible outputs: defining five career levels in the supply chain, describing skills requirements by technical area, accessing a compendium of opportunities for education and training for skills needed and refining or creating job descriptions. In the long term, because of this approach, countries can develop a detailed plan for HSCM professionalization, including designations, SCM professional standards and education standards. This process will develop specific designations and career paths and a matching repository of job descriptions and education opportunities. It will also facilitate the creation of competency-based assessments.
Comparing the existing HR system for SCM at the organizational level to the HR4SCM TOC requirements uncovers gaps in the existing system and enables stakeholders to understand what is required to optimize worker performance. Using the HR4SCM TOC as a diagnostic tool enables development of interventions to improve identified gaps and the tool includes suggested indicators for monitoring improvements.
In terms of generalizability, although the SCM Professionalisation Framework is specific to health SCM, it could be broadened and adapted for the humanitarian logistics sector. The HR4SCM TOC and labor market analysis tools of this approach can be applied in all sectors of SCM workers, including commercial and humanitarian sectors. Implementing this approach can improve human resources available during humanitarian situations. Applying this approach could also improve organizational-level factors, including staffing, skills and working conditions, at organizations employing humanitarian workers.
4.5 Limitations
Although we engaged with HSCM representatives from various sectors to develop the three tools described in this approach, we did not engage all HSCM actors. As such, certain alternative perspectives might be missing. Due to the time required to make necessary changes identified through this approach, the ultimate impact of our approach is still to be demonstrated. Due to the nature of this iterative approach, we did not pre-define an overarching set of metrics for the comprehensive approach described in this paper, limiting our ability to measure impact.
5. Conclusion
An adequate pool of qualified, competent workers who effectively manage the health supply chain is critical to ensure that a reliable, cost-effective supply of quality medicines are available to meet UHC and development goals. Using the PtD systems thinking approach enables countries to clearly define roles and responsibilities for their public health supply chain workforce. Adopting the PtD SCM Professionalisation Framework allows countries to define the technical areas required in the supply chain and the skills needed at each level. By moving from a limited focus on individual- and organizational-level interventions to comprehensively considering all elements influencing organizational and worker productivity, this approach has the potential to optimize HR systems, improve workforce development initiatives and optimize individual workforce performance. Program managers and national stakeholders should consider the PtD systems thinking approach to workforce development to strengthen the workforce managing public health supply chains.
The PtD experience of implementing a systems thinking approach to workforce development in Rwanda offers critical lessons for other countries aiming to assess and improve their HSCM workforces and is perceived to have had broad and beneficial impacts, although formal evaluations are still needed. Adopting this approach can help governments and partners achieve progress beyond what is possible from reactive, discrete individual interventions. Future research should consider defining a set of overarching indicators to measure progress of this systems thinking approach to HSCM workforce development.
Acknowledgement
The research described in this article is the result of a collaborative effort between the People that Deliver (PtD) Initiative, USAID Global Health Supply Chain Program – Procurement and Supply Management (GHSC-PSM) project and USAID. USAID provides funding for both PtD and GHSC-PSM. The views and opinions expressed in this paper are those of the authors and not necessarily the views and opinions of the United States Agency for International Development.
Note
As the global technical leader in human resources for HSCM, People that Deliver (PtD) builds on the experiences of its coalition members from 28 organizations to advocate for change at the global and country-level. PtD’s unique feature is that coalition members are the vehicles for the provision of services and funding. This results in stronger and more sustainable systems for developing, recruiting and retaining a qualified health supply chain workforce.
References
Supplementary material
The supplementary material for this article can be found online.