The purpose of this paper is to propose a novel evidence-based Haddon matrix that identifies intervention options for organizations and governments responding to an epidemic in a developing economy.
A literature review of articles published within a year of the cholera outbreak in Haiti. Two separate types of literature sources are used – academic and non-academic – to apprehend the value and role of interventions implemented and/or identified.
The Haddon matrix helps break down the challenges involved in the containment of an epidemic into smaller, manageable components. This research shows that the matrix enables visualization of past evidence, help dissect various informational sources, and increase collaboration across humanitarian organizations. It will also serve as a building block for academics to identify new research directions to respond to epidemic outbreaks.
The analysis focuses on the cholera epidemic in Haiti. Future work will be directed to generalize the identified recommendations and insights to a broader context.
This paper presents an evidence-based Haddon matrix that infers recommendations and insights based on past evidence for each phase (pre-event, response, and post-event) and factor (agent, host, physical environment, and socio-cultural environment) of an epidemic and for various stakeholders (humanitarian organizations, governments, and academics). The matrix provides a structured framework to identify interventions and best practices to address challenges during an epidemic outbreak.
1. Introduction
The frequency and intensity of disasters have increased over the last few decades creating a global concern for effective disaster management. The annual average number of deaths resulting from natural disasters in the years 2003-2012 was 106,654 (Guha-Sapir et al., 2014). The cost of disasters is comparatively larger in developing economies than in their developed counterparts (Noy, 2009). Dilapidated living conditions with poor water and sanitation systems exacerbate this issue. The recent episodes of epidemic outbreaks have created a large global burden on humanitarian efforts. The 2014 Ebola outbreak in West Africa affected roughly 25,000 people and claimed approximately 10,000 lives in Guinea, Liberia, and Sierra Leone (CDC, 2014). The 2008 cholera outbreak in Zimbabwe reached its peak with over 8,000 cases reported in a single week. As of 2013, cholera alone represented an estimated 1.4-4.3 million cases, and 28,000-142,000 deaths per year worldwide (World Health Organization, 2014).
This study develops an evidence-based tool using the Haddon matrix concept to respond to the dire needs caused by an epidemic in a developing country. The nature of the response varies depending on the nature of the disaster. Slow-onset disasters permit organizations to plan ahead of time, while sudden-onset disasters demand quick response within a very short timeframe. Most humanitarian organizations have specialized areas of expertise, such as water and sanitation or healthcare services (OCHA, 2014). This makes coordination among responding organizations and other actors, such as logistical service providers, critical (Bealt et al., 2016). For example, Apte et al. (2016) emphasize the core competencies and capabilities of the US military that are useful during disaster response operations. Nonetheless, the degree of collaborative action among responding organizations seems to be poor during the disaster response phase. Further, evidence of learning from past disaster events appears low. Approximately two years prior to the cholera outbreak in Haiti, Zimbabwe experienced what was termed the “worst cholera epidemic in Africa” (Mason, 2009). Zimbabwe’s poor standards of healthcare were similar to those in Haiti during the October 2010 cholera outbreak (Ahmed et al., 2011; Walton and Ivers, 2011). However, the evaluation reports examined in this research indicate that only a few large NGOs, such as Médecins Sans Frontières (MSF) utilized the lessons learned from the experience in Zimbabwe when responding to the Haitian outbreak (Bergeri, 2011). As shown by these examples, there is not enough collaboration between humanitarian organizations. The lack of learning from past evidence when responding to an epidemic outbreak motivated us to develop a tool that can address this issue. Chamberlin, Efron and Moore (2015) emphasize the need for “simple, practical, proof-of-concept” policy analysis tools that could enhance a “decision-maker’s ability to systematically assess the potential interventions” when it comes to an epidemic outbreak scenario. Thus, this study provides a simple and practical methodology to improve the capability of policymakers to assess the value and suitability of past interventions for future epidemic situations as they arise.
The research contributions of this paper are twofold. First, we propose a novel evidence-based matrix that identifies intervention options for humanitarian organizations and governments responding to an epidemic in a developing economy. The proposed Haddon matrix (Haddon, 1968) can be used as a planning tool to understand, prepare for, and respond to an epidemic. In this paper, evidence extracted from academic and non-academic literature sources is used to populate the Haddon matrix. We look at the context of the 2010 cholera outbreak in Haiti. The benefits and importance of learning from evidence have been emphasized in humanitarian action (Bradt, 2009; de Goyet et al., 2011; Dijkzeul et al., 2013) and in the academic literature (e.g. the 2013 special issue of the Disasters journal was devoted to evidence-based action in humanitarian crises). Second, this paper intends to systematically display evidence from real epidemic-related interventions, thereby reducing the “lack of understanding among academics” about real humanitarian operational issues (Pedraza-Martinez et al., 2011) and healthcare needs in developing countries (McCoy and Johnson, 2014; McCoy and Lee, 2014).
To our knowledge, this paper is the first to use an evidence-based Haddon matrix that infers recommendations and insights for each phase (pre-event, response, and post-event), factor (agent, host, physical environment, and socio-cultural environment) of a disaster, and for various disaster stakeholders (humanitarian organizations, governments, and academics) of a disaster. The developed matrix provides a structured framework to identify interventions and best practices to address challenges during an outbreak. Hidalgo (2011) asserts that “new frameworks and approaches” are needed in order to overcome “weaknesses in coordination across sectors.” The proposed Haddon matrix responds to that need, and can serve as a cornerstone to enhance coordination among humanitarian organizations, governments, and academics to improve their understanding of the required interventions during an epidemic outbreak. The framework can be used to reduce social costs (Holguín-Veras et al., 2013) associated with the response to such a crisis in a developing economy. Kraiselburd and Yadav (2013) argue that it is vital to develop new “research frameworks of analysis which would then become the cornerstones for policy advice to those who design, operate, or finance” health care supply chains. The proposed method can be used as a building block for academics to identify research directions that support decision making during epidemic outbreaks.
The rest of this paper is organized as follows: Section 2 briefly describes the humanitarian response challenges faced during Haiti’s cholera epidemic and explains the selection criteria of the data sources used in this research. Section 3 introduces the Haddon matrix concept, its application in various contexts, and presents the newly developed Haddon Matrix. Section 4 describes key observations extracted from the new evidence-based Haddon matrix and identifies intervention options for future epidemic scenarios. It also identifies potential research directions for academics in the humanitarian and disaster management fields. Section 5 summarizes the contributions of this research, discusses some of its limitations, and suggests avenues for future research.
2. Use of evidence for humanitarian response
In the first part of this section we identify challenges faced in humanitarian response efforts. Section 2.2 gives a brief overview of the Haitian cholera epidemic outbreak. Section 2.3 analyzes the importance of evidence-based decision making, while Section 2.4 defines the selection criteria for the sources of evidence used in this research.
2.1 Challenges in humanitarian response
The nature of the challenges faced during a disaster response effort varies with the type of disaster (Noji, 2005). The United Nation’s (UN) Logistics Cluster identifies three categories of disasters based on the type of intervention: slow-onset, sudden-onset, and complex emergencies (WFP, 2013). Decision making is tough for responding organizations and governments in disaster situations because of the need to address uncertainties while making plans for future requirements (WFP, 2013).
Various mechanisms have been implemented to improve information exchange among humanitarian organizations and responding governments. These mechanisms can be web-based services, such as the UN website for sharing humanitarian information called Relief Web (2014). Other initiatives include Non-Government Organization (NGO) consortiums, such as the Comité de Coordination des ONGs en Haiti (CCO) (2013), a group of 44 NGOs that collaborate for policy making, coordination, and information sharing in Haiti. However, even with the cluster system put in place by the UN during the 2010 Haitian earthquake, coordination between UN clusters was not efficient, and effective decision making was a challenge (Altay and Labonte, 2014). Similarly, de Goyet et al. (2011) state that “there is a strong consensus that the response from all sectors was chaotic and poorly coordinated in Haiti during the earthquake in 2010.” Referring to Haiti’s cholera outbreak, CCO (2013) regrets that “no NGOs contributed to the development of the national plan to eliminate cholera, even though they played a key role in the response to recent outbreaks.” Further, as stated in the introduction, the response to Haiti’s outbreak showed very little evidence of applying lessons learned from the earlier cholera epidemic in Zimbabwe (Bergeri, 2011). This motivated us to develop an evidence-based tool that proposes options for effective decision making in the case of an epidemic occurring in a developing economy. The evidence-based Haddon matrix developed in this paper can be easily used across various responding organizations and governments to help prioritize objectives and allocate resources in a coordinated fashion during a sudden-onset disaster.
2.2 Background for the 2010 cholera epidemic in Haiti
In this research, we use the 2010 cholera epidemic in Haiti as a case study. Haiti had not experienced cases of cholera for over a century (Chin et al., 2011; Walton and Ivers, 2011). But in October 2010, cases of cholera were reported a few months after the country was hit by a 7.0-magnitude earthquake (Barzilay et al., 2013). As cholera has short incubation periods ranging from two hours to five days (World Health Organization (WHO), 2004), the disease spread to every province of Haiti within weeks. By the end of the year, more than 150,000 cases and 3,500 deaths were reported (Andrews and Basu, 2011).
2.3 Evidence-based decision making in humanitarian response
Bradt (2009) defines evidence as “data on which a judgment or conclusion can be based.” Clarke and Darcy (2014) define evidence as “information that helps prove/disprove the truth of a specific proposition.” In the humanitarian logistics literature, Pedraza-Martinez et al. (2013) use the term evidence to distinguish between qualitative and quantitative information components that were obtained through theoretical research (quantitative) and humanitarian organizational inputs (qualitative). The ability to learn from evidence is viewed as critical in the humanitarian context (see e.g. Bradt, 2009; Dijkzeul et al., 2013). Clarke and Darcy (2014) stress the need for evidence-based decision making in humanitarian assistance.
The idea of using evidence for decision making purposes originates from the concept of evidence-based medicine defined as “using the best possible evidence in order to answer a clinical question” (Rosenberg and Donald, 1995). The concept of evidence-based decision making has been used in the humanitarian context to determine the allocation of financial contributions to countries affected by disasters (ALNAP, 2013; Clarke and Darcy, 2014). Evidence-based decision making ensures effectiveness and accountability of humanitarian assistance, which is essential due to resource limitations and high level of uncertainty in disaster response operations (ALNAP, 2013; Clarke and Darcy, 2014). To our knowledge, there exists no evidence-based study designed to support the response to sudden-onset disasters, such as epidemic outbreaks.
2.4 Evidence sources and selection criteria
The interpretation of evidence is challenging in the humanitarian context due to the particular requirements and approaches of humanitarian organizations (ALNAP, 2013). For example, Rencoret et al. (2010) observe that key concepts, such as displacement and affected/non-affected populations, are subject to various interpretations depending on who gathered the information. In this study, we define evidence as the available quantitative and qualitative information from a past disaster that can help identify interventions for a future epidemic outbreak. We use the academic and non-academic literature about a past epidemic as primary evidence sources. The purpose of this study is to introduce the Haddon matrix as a useful coordination tool for stakeholders when responding to a future epidemic scenario. In this study, we distinguish academic from non-academic references. Future studies could refine the categories of literature sources to include opinions, case reports, case series, ecological studies, cross-sectional studies, randomized controlled trials, and meta-analysis.
As in recent desk-review articles about epidemics and other types of disasters (see e.g. Altay and Labonte, 2014; Kouadio et al., 2012), we select sources published within a year of the disaster. For data triangulation purposes (Eisenhardt and Graebner, 2007), we use two separate types of evidence – academic and non-academic sources – to apprehend the value and role of interventions implemented and/or identified in the past.
Non-academic evidence sources in the humanitarian literature can come in various forms, such as needs assessments, evaluation reports, after action reports, and lessons learned reports. In selecting non-academic sources, we follow the selection methodology used by Altay and Labonte (2014), and searched for documentation on the cholera response effort in Haiti in the Active Learning Network for Accountability and Performance in Humanitarian Action database. Ten non-academic sources were collected, consisting of evaluation and “lessons learned” reports about the cholera outbreak in Haiti prepared by various humanitarian organizations. Sources that did not discuss any interventions relevant to the outbreak were not included. These reports were compiled by organizations based on multiple data sources: humanitarian agency performance in health facilities (Bergeri, 2011), interviews with Haitian institutions, international agencies, and affected communities (Hidalgo, 2011; de Goyet et al., 2011; Wall and Chery, 2011; Crenn, 2011; MOFA-Dutch, 2011), project documentation, sampled beneficiary surveys and questionnaires (Crenn, 2011), and desk studies (MOFA-Dutch, 2011).
For academic sources, we conducted a Google scholar search to retrieve peer-reviewed articles about the Haitian cholera epidemic. The search was conducted using the keywords, Haiti, cholera and response, and resulted in 35 academic sources. These sources were then analyzed in order to assess the interventions that are useful for an epidemic outbreak in a developing country. The next section introduces the Haddon Matrix, which we utilize to organize the findings obtained from the analysis of academic and non-academic evidence sources.
3. Haddon matrix concept
The Haddon matrix concept was introduced by William Haddon as a tool to analyze factors that affect traffic safety injury and prevention (Haddon, 1968). Table I is a general version of the Haddon matrix, which consists of four columns and three rows. The rows stand for the phases of a disaster s, while the columns represent various influencing factors during a disaster. Sections 3.1 and 3.2 describe the significance of each column and row in the matrix.
The Haddon matrix helps “dissect a problem into phases of a disaster and the contributing factors, and can be applied as a practical, user-friendly interdisciplinary brainstorming and planning tool to understand, prepare for, and respond to a broad range of public health emergencies” (Barnett, Balicer, Blodgett, Fews, Parker and Links, 2005). The Haddon matrix was also used in other epidemiological studies, such as the spread of influenza pandemics, emergency preparedness, and drowning prevention (Barnett, Balicer, Blodgett, Fews, Parker and Links, 2005; Barnett, Balicer, Lucey, Everly, Omer, Steinhoff and Grotto, 2005; Guevarra, 2011). Barnett, Balicer, Blodgett, Fews, Parker and Links (2005) extended the Haddon matrix concept to address a hypothetical situation of SARS and “dirty bomb” attacks. The authors illustrate the effectiveness of the Haddon matrix as a planning tool to better react to such public health threats in the USA. The aforementioned examples illustrate the versatility of the Haddon matrix and its wide applicability. The ability to dissect an event into smaller segments and systematically identify preparedness and intervention strategies is a key benefit of this matrix. While most former studies utilizing the Haddon matrix concentrate on influenza outbreaks, this study focuses on cholera, a disease that has the potential to kill within few hours if left untreated. The ability to decompose an event motivated us to use the Haddon matrix, it provides pointed recommendations for each phase and factor to the various stakeholders and responding organizations.
3.1 Factors relevant to the disaster event
The columns in the Haddon matrix represent the main four factors relevant to any disaster: host, agent, physical environment, and socio-cultural environment. The host is the person that is susceptible to injury and the agent is the primary cause of occurrence of an event. In the case of an epidemic, the agent is the disease-causing virus. The physical environment comprises physical infrastructure and mechanisms that must be in place to effectively address a disaster. For example, during an epidemic the physical environment includes requirements for healthcare facilities, availability of healthcare professionals, and availability of drugs inter alia. The features related to physical environment are typically poor in developing or least developed economies. The socio-cultural environment encompasses social and cultural practices as well as laws and regulations that affect each phase of the disaster. Other requirements such as funding needs, effective transition mechanisms, and related policies fall under this category. The socio-cultural environment factor helps understand the macro-level needs of governments and humanitarian organizations to provide an efficient response. For example, there might not be a system in place to increase the socio-cultural awareness of humanitarian organizations responding to a disaster in a developing country. This would adversely affect the entire response effort, because effective communication between organizations and the community is crucial (Wall and Chéry, 2011).
3.2 Phases of concern (rows in the Haddon matrix)
Disaster management is “the coordination and integration of all activities necessary to build, sustain and improve the capabilities to prepare for, respond to, recover from, or mitigate against threatened or actual disasters or emergencies, regardless of cause” (Department of Homeland Security, 2007). Mitigation, preparedness, response, and recovery are the key phases in the disaster management cycle, and are called the phases in the Haddon matrix terminology.
The pre-event phase in the Haddon matrix involves the mitigation and preparedness aspects of a disaster cycle. In case of a disease outbreak, this phase focuses on preventing the agent or virus from reaching the susceptible host or human body. This phase includes activities, such as monitoring for possible indications of a disease outbreak, maintaining satisfactory health and sanitation standards, improving awareness, and conducting accrued surveillance among populations at risk. This is crucial since developing countries may lack surveillance mechanisms and proper sanitation/infrastructure facilities, which exacerbate the consequences of the epidemic.
The response phase takes place when the agent interacts with the host, i.e. when a virus enters the body of a human. There is ample opportunity for exacerbates for intervention in order to prevent severe infection or death of the host. Early identification of a host should ideally translate into early treatment mechanisms so that the health of the host does not deteriorate further. Typically, this is the phase when responding organizations need to create an environment that contains the disease and provide access to treatment for the affected populations.
The post-event phase is when damage has been done and the affected community needs to transition from response to recovery. At this stage, it is crucial to maximize the impact of the recovery strategies to help the community move on from the disaster response phase. The post-event phase involves decisions taken to minimize further harm to human life, such as evacuation and improvement of infrastructure, and to return the situation back to normal as soon as possible.
The proposed Haddon matrix makes it possible to identify decision-making challenges and opportunities specific to each phase of the disease outbreak. This gives a better overview of possible intervention strategies and policies that can alleviate the devastating consequences of epidemics. In previous studies based on the Haddon matrix concept (Barnett, Balicer, Blodgett, Fews, Parker and Links, 2005; Barnett, Balicer, Lucey, Everly, Omer, Steinhoff and Grotto, 2005), limited evidence from past disaster contexts was used to partially inform either the response or post-disaster phase of a disaster. In contrast, we provide in this study evidence to inform every phase, pre-event, response, and post-event of the epidemic management cycle in a developing country. Furthermore, while all previous studies focused on providing insights to public health decision makers only, our study provides insights to humanitarian response organizations, governments, and academics.
3.3 Evidence-based disaster decision-making tool
de Goyet et al. (2011) state that “lessons learned tend to focus on resolving what did not work so well” and on the “considerable achievements of the humanitarian community.” To ensure an effective response, it is essential to base decisions on these “lessons learned” or best available evidence. The literature on humanitarian response to epidemics stresses the importance and value of learning from past evidence and highlights how seldom it is done.
Various humanitarian organizations have developed response tools to suit their respective objectives. But there is a disconnect between organizations as these tools may not serve a common objective (Bradt, 2009; Darcy et al., 2013; Dijkzeul et al., 2013). There is concern about the extent to which humanitarian partners can learn from each other without a common database that enables joint decision making (Mills, 2005). If communicated appropriately via a common platform evidence from past disaster scenarios can be used to strengthen the trust between humanitarian organizations, governments, and academics. This motivated us to develop an evidence-based Haddon matrix restructured to address epidemics in developing countries. The structure of the proposed Haddon matrix and its ability to decompose complex events will facilitate the collaboration across responding organizations and governments, the prioritization of the objectives and challenges, and the determination of the interventions to be jointly implemented, and the identification of future research directions for academics. The next section presents an explanation of the restructured Haddon Matrix developed in this paper.
3.4 Modifications to the standard Haddon matrix
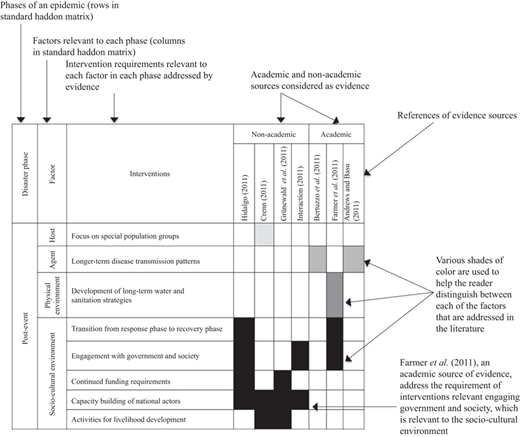
We have incorporated several changes in the format of the standard Haddon Matrix presented in Section 3 in order to better visualize evidence, inform multiple stakeholders, and cover each phase of the disaster management cycle. Figure 1 gives a description of how the novel Haddon Matrix can be read.
A key modification is that the factors, displayed as columns in the standard Haddon matrix, correspond to rows in the new Haddon Matrix. The rows of the new Haddon matrix are first broken down by disaster phases. The rows are then further decomposed with respect to the four factors. Finally, the factor rows are subdivided per type of intervention. The columns in the new Haddon Matrix correspond to the type (academic or non-academic) evidence sources. The modifications in the display of the proposed Haddon matrix are needed due to our data triangulation approach, so that academic and non-academic evidence sources and insights can be easily and visually distinguished. The recommendations and insights that we derive for stakeholders are presented in Section 4.
We build the new Haddon matrix as follows. First, evidence sources are selected from academic and non-academic sources using the approach described in Section 2.5. We then search interventions reported in the evidence sources, and identify the factor and phase of the Haddon matrix to which the interventions are related to. Next, we map the evidence sources and the identified interventions to the new Haddon matrix, which allows us to subsequently provide insights and recommendations for various stakeholders (humanitarian organizations, governments and academic community), each phase of the disaster, and each factor relevant to an epidemic outbreak. The complete Haddon matrix developed using this process is displayed in Table II. Chamberlin, Efron and Moore (2015) note that the decision makers could dynamically update such a matrix by drawing “from all available data, such as from published reports, internal situational reports, operational updates, views of subject-matter experts, and so on.” The method proposed in this paper will prove particularly effective when decisions must be made using a brief review of the available evidence sources.
4. Discussion of intervention recommendations and insights
In this section, we present the recommendations and insights drawn from the new Haddon matrix. This section is organized per disaster phase: pre-event, response, and post-event. The “Interventions” column in Table II summarizes the various interventions drawn from each source of evidence. We describe the interventions with respect to the factors, phases, and relevant stakeholders. We also compare the extent to which academic and non-academic evidence sources agree or not on the aforementioned interventions. Additionally, it can help identify new research directions based on practical challenges highlighted in non-academic evidence sources.
4.1 Pre-event phase
The pre-event phase includes interventions concerning the mitigation and preparedness options for a potential epidemic outbreak. It is clear from Table II that despite the neglected health conditions in Haiti, very few academic and non-academic sources discuss interventions for the pre-event phase. Those that do so stress the potential risk of an outbreak and focus on the interventions relevant to the physical environment factor. In this phase, academic and non-academic sources agree that the risk of an outbreak, even though eminent in a country like Haiti, was severely underestimated.
4.1.1 Physical environment factor
Bergeri (2011) and Farmer et al. (2011) both emphasize that the risk assessment capability and preparedness for an epidemic outbreak were insufficient in Haiti. Given that Haiti’s health infrastructure and sanitation capabilities were already dwindling in the face of the earthquake, “the risk of a diarrheal epidemic in this context was overly downplayed” (Bergeri, 2011). Farmer et al. (2011) further highlight the need for a global medicine stockpile so that developing countries facing a sudden epidemic outbreak would be able to benefit from quick access to medicine. Ryan (2011) underscores the importance of being prepared to use vaccines as an effective intervention option in reactive epidemic settings such as Haiti. However, they also bring to attention that “such use [of vaccines in a country like Haiti] would first require additional field and cost-effectiveness evaluations and intricate planning and commitment.” More specifically, they put forward a series of questions that should be addressed to successfully deal with an epidemic outbreak: “Would an international stockpile of vaccine be beneficial? Who would support and manage it? What would be the triggers for its use? How would its benefit be measured? […] What are the obstacles? How can we improve our track record?”
4.1.2 Insights for practitioners and academics
The few interventions discussed in the collected evidence focused on the physical environment for the pre-event phase. Early detection of a potential outbreak and having medical options in place are key concerns. The concerns brought up by Bergeri (2011), Farmer et al. (2011), and Ryan (2011) are most relevant for governments of countries that are at risk of epidemic outbreaks. However, practical implementation of such medical interventions will have to be encouraged and/or sponsored by organizations such as WHO (as for the response strategies designed for pandemic influenza Jennings et al., 2008). In this phase, NGOs (see e.g. OXFAM (2012)) could help governments assess the risk of an epidemic outbreak by developing medical and detection guidelines. Humanitarian organizations must try to alleviate the risk of epidemic outbreaks in vulnerable countries (Bergeri, 2011).
The academic community could contribute to this phase by developing tools and models that would help countries and/or organizations assess the risk of an epidemic outbreak. Facility location and resource allocation models are commonplace in humanitarian research. However, the review of the literature indicates that models for vaccine allocation have only been developed for certain diseases, such as polio or influenza (Jennings et al., 2008; Tebbens et al., 2010). There have been a few recent successful responses to cholera outbreaks in vulnerable communities (i.e. Iraq and South Sudan Lam et al., 2017; Parker et al., 2017) using oral vaccination. However, poor sanitary conditions in rural countries like Haiti put populations at higher risk of contracting cholera despite vaccination (Matias et al., 2017). Therefore, additional studies are required to design medical intervention strategies that tie together earlier successful strategies in resource-constrained developing countries (such as in Iraq and South Sudan).
4.2 Response phase
Table II indicates that most academic and non-academic sources focus on interventions pertaining to the response phase. Interventions concerning the physical environment factor draw most attention. Non-academic evidence sources also cite interventions for the host and socio-cultural environment factors. Academic evidence sources pay a lot of attention to disease transmission patterns relevant to the agent. While academic and non-academic sources agree on the physical environment-oriented interventions, they however emphasize different interventions for the other factors.
4.2.1 Host factor
Only non-academic evidence sources specifically analyze interventions relevant to the host factor. For example, non-academic sources argue that special attention should be given to different patient groups, including children, elderly, and pregnant women. In the MSF treatment centers, the provision of isolated care and therapy for pregnant women led to fruitful outcomes (Bergeri, 2011). Data collection and surveillance are critical in order to assess the number of patients and criticality of the epidemic outbreak (Bergeri, 2011). However, it is reported that the data collection process was restricted to health facilities operated by certain organizations (e.g. MSF).
4.2.2 Agent factor
The interventions concerning the agent factor are predominantly discussed by academic sources, and are associated with the infectivity and transmission (Piarroux et al., 2011; Bertuzzo et al., 2011; Andrews and Basu, 2011; Tuite et al., 2011) of the disease-causing vector. To understand disease transmission patterns, lab tests need to be carried out on a continuous basis (Bergeri, 2011). However, in reality, very few laboratory confirmations of the cholera outbreak were carried out and no regular tests were conducted during the initial months of the outbreak (Bergeri, 2011). Further, MSF (2011) reiterates the difficulty to predict the trajectory of cholera transmission in Haiti. Such difficulties in accurately apprehending the transmission pattern of the disease led to an insufficient distribution of medical aid in some parts of the country (MSF, 2011).
4.2.3 Physical environment factor
Both academic and non-academic sources agree on a number of interventions concerning the physical environment factor. This includes, for example, the introduction of preventive and curative activities, the development of treatment protocols, the identification of a coherent sanitation strategy, the training of staff, and the establishment of proper water and sanitation facilities. Bergeri (2011) explains that the delays in establishing “treatment protocols”, such as introducing zinc to treat kids early in the outbreak, resulted in the overuse of drugs available in limited quantities. However, critical interventions, such as the development of decentralized urban/rural strategies involving, for example, the opening of health facilities, are stressed by non-academic sources only. The economic and infrastructure disparity between urban and rural Haiti makes it necessary to have a “decentralized rural strategy.” But the implementation of such strategies was not in place until weeks after the outbreak (Bergeri, 2011). Some NGOs, such as those funded by the European Commission for Humanitarian Aid Office, are said to have personnel who lacked the required skills for some operations and who could only cope with adversarial situations “with varying levels of success” (Grünewald et al., 2011). The limited access to qualified personnel was in part due to the earlier earthquake, which exacerbated the impact of the scarcity of some key resources (Bergeri, 2011). As it can be inferred from the above, the interventions discussed in the academic and non-academic sources differ significantly.
4.2.4 Insights to practitioners and academics
The intervention recommendations for the response phase call for the collaboration of humanitarian organizations, governments, and relevant international organizations. Interventions concerning the host factor, such as the focus on special patient groups and the collection of patient data, need to be implemented across humanitarian organizations as uniformly as possible. Better coordination among agencies to implement these interventions is crucial. Based on the above-presented observations, it appears that academics should strive to develop operational strategies for humanitarian organizations, particularly with respect to the efficient handling of special patient groups and implementation of differentiable urban/rural strategies.
4.3 Post-event phase
In the post-event phase, almost all the surveyed non-academic sources focus exclusively on the socio-cultural environment. Academic sources primarily analyze interventions for the agent and the disease transmission patterns.
4.3.1 Agent factor
Concerning the agent factor, academic evidence sources mostly seem to develop simulation models to understand the impact of various medical interventions on long-term disease transmission patterns (Andrews and Basu, 2011; Bertuzo et al., 2011). On the other hand, non-academic sources stress the need for effective mechanisms to deliver humanitarian assistance to special population groups. For example, interventions conducted by humanitarian organizations such as HelpAge Haiti (Crenn, 2011) aim at providing special care to elderly patient groups.
4.3.2 Socio-cultural environment factor
Interventions for the socio-cultural environment are recommended by non-academic sources and focus on the need and challenge of raising funds after the disaster. The ability to smoothly transition from the response phase to the recovery one will be contingent on the availability of funding for development projects. Furthermore, donors should use funding mechanisms that do not hinder operations of humanitarian organizations when moving from the response phase to long-term recovery and development (Grünewald et al., 2011).
4.3.3 Insights for practitioners and academics
The post-event phase is centered on the move from response to long-term revival of the society and community. In the post-event phase, organizations face a shift of “focus from speed to cost reduction” (Tomasini and Van Wassenhove, 2009). Consequently, this phase tends to be neglected (Cozzolino et al., 2012), which points out to the need for sustained involvement of humanitarian actors, governments, and other international agencies beyond the response phase. As stated in Hidalgo (2011), “The humanitarian community, in coordination with development actors, needs to reengage with the new government and the Haitian society and take advantage of institutional changes – to adapt its approach, better communicate its concerns and jointly define an action plan that addresses humanitarian priorities and provides clarity for transition.” This highlights the need for a bottom-up approach to understand humanitarian and cross-organizational collaboration needs. The academic community should develop research paths that benefit the long-term development of a country recovering from an epidemic. Academics should not only limit their efforts to the study of disease transmission patterns, but also undertake research allowing for the development of effective funding operations and livelihood development addressing the challenges pointed out in Tomasini and Van Wassenhove (2009) and Cozzolino et al. (2012) and allowing for the transition from the response phase to the post-disaster/recovery phase.
5. Conclusions
Epidemic outbreaks create a challenging environment in countries with scarce resources and poor sanitation infrastructure. An epidemic outbreak in a developing country demands the involvement of humanitarian organizations and governments. Past epidemic scenarios show that aid coordination systems need to improve across agencies and the UN clusters as a whole (Bergeri, 2011; Hidalgo, 2011). This points to the value of developing an evidence-based tool that shows the value and nature of interventions, helps prioritize them, and facilitates cross-collaboration among responding entities. This research shows that academic and non-academic actors agree that vulnerable countries like Haiti often underestimate the risk of an epidemic and are not sufficiently prepared to deal with it.
Using the 2010 cholera outbreak in Haiti, we propose an evidence-based Haddon Matrix, which analyzes intervention options for an epidemic outbreak in a developing country. We use data triangulation and mix academic and non-academic sources to build a novel evidence-based Haddon matrix.
The Haddon matrix can be used to infer intervention insights and recommendations for each phase, factor, and stakeholder of an epidemic outbreak. More precisely, the Haddon matrix developed in this paper: permits us to break down and dissect the complex problem of containing an epidemic into smaller, more manageable components; helps visualize evidence for each of those components; facilitates collaboration across responding organizations and the prioritization and coordination of their interventions; and serves as a building block for academics to identify research directions that could eventually improve the decision-making process during epidemic outbreaks. The matrix developed in this paper is a flexible tool that can accommodate various time constraints. If short on time, decision makers could utilize it to make quick decisions. With more time available, they could complement the matrix via an extended data collection and consultation with subject experts.
5.1 Implications for academia and practice
In the pre-disaster phase, governments of countries at risk of epidemic outbreaks and humanitarian agencies should improve their preparedness, which includes access to global medicine stockpiles and analysis of the usefulness of vaccines. The academic community could contribute in this respect by developing models estimating the effect of vaccines on the spread of epidemics. Additionally, procedures designed to detect an epidemic at its onset are also needed.
In the response phase, both academic and non-academic sources recognize the need for physical environment-oriented interventions involving, for example, the development of preventive and curative activities, treatment protocols, and sanitation strategies, as well as training of medical staff. However, while academic sources are primarily insightful about models for disease transmission patterns, non-academic sources point out that the lack of laboratory testing mechanisms on the ground should be remedied in priority. The lack of tests does not allow the tracking of the spread of the disease and the efficient allocation of scarce medical resources. It is encouraging to see that researchers have identified such needs and are now developing specific research directions, for example, for field level laboratory management during epidemics (Vybornova and Gala, 2016). Non-academic sources also highlight the significance of the limited availability of qualified personnel. Since economic and infrastructure conditions are often worst in the rural parts of developing countries such as Haiti, it is critical to have a decentralized rural strategy. However, this study reveals that differentiated strategies were hardly implemented even weeks after the outbreak.
For the post-event phase, socio-cultural interventions are crucial, and include the engagement of government and society, the search for funding, and the capacity building of national actors. This will require coordination among humanitarian organizations, governments, and other international agencies to secure proper funding in order to aid the affected area in transitioning from the response phase to effective recovery. At that stage, it is essential that humanitarian organizations engage with the government and society and communicate clearly their action plans and priorities. The academic community needs to develop research agendas that will look into non-profit funding mechanisms for the immediate response phase as well as for the long-term development of a country recovering from an epidemic.
5.2 Limitations
It appears that studies using evidence from past disasters to inform future interventions are often based on a single disaster case study (see e.g. Chamberlin, Efron and Moore, 2015; Chamberlin, Okunogbe, Moore and Abir, 2015 – Ebola Epidemic; Acosta et al., 2015 – Hurricane Sandy). Our analysis is also focused on the context of a particular disaster, the cholera epidemic in Haiti. However, we believe that the approach presented in this paper will help future researchers expand the use of the modified Haddon matrix to other epidemic- and non-epidemic-related studies.
5.3 Future research directions
The conceptual methodology developed in this paper, as well as the derived recommendations, could be easily extended to other disaster contexts. The cholera epidemic in Haiti, one of the largest outbreaks in the recent past, is comparatively well-documented. As more information becomes available for other epidemics, such as the Ebola outbreak in West Africa, an extension of this study could consider multiple epidemic outbreaks. This could allow us to distinguish the idiosyncratic recommendations for the Haitian cholera outbreak from the more general ones that could apply across epidemic types and developing economies. Additionally, we could expand the period for which evidence sources are collected and analyzed.
The interventions and insights presented in this study are not categorized based on the type of responding agency (e.g. medical NGO, local NGOs, philanthropic organizations, etc.). Similarly, the insights provided to researchers have not been specifically broken down by research areas (e.g. epidemiology, healthcare operations, humanitarian, and not for profit operations). These could be useful extensions, but they would also introduce an additional dimension to this study and would make the visualization of the Haddon matrix more complicated. Finally, while evidence sources are extracted in this study from online academic and non-academic publications, future updates of the Haddon matrix by on-ground decision makers could “provide comprehensive and likely uncover new information” (Chamberlin, Okunogbe, Moore and Abir, 2015).