This study aims to investigate the coevolution of supportive social ties and psychological distress within The Phoenix, a sober active community. It also aims to disentangle two concurrent processes: whether psychological distress influences the formation of social ties (social selection) or whether peer relationships influence individual distress levels (social influence) over time.
Longitudinal social network data were collected from members of The Phoenix in Denver and Wichita (n = 23) across two waves separated by one year. This study used the Simulation Investigation for Empirical Network Analysis (SIENA) framework to simultaneously model structural network dynamics and changes in psychological distress.
Network ties were characterized by reciprocity and clustering. A significant negative selection effect was identified (PE = −0.37, p < 0.05): members with lower psychological distress were more likely to be nominated as supportive partners, while those with higher distress were less likely to be selected. No evidence of peer influence on psychological distress was observed over the one-year period.
Limitations include small network sizes and a two-wave design, which restricted model complexity. Future research should incorporate additional waves, larger networks and mixed-method approaches to capture nuanced changes in mental health and social integration.
Findings suggest that members with higher psychological distress are less likely to be selected as supportive ties, potentially isolating those most in need of connection. “Structured socialization” strategies, such as assigned mentorships or care circles, could be implemented to proactively integrate members with higher distress levels who might otherwise be filtered out by the community’s selection mechanisms.
While recovery communities provide vital protection, they can also function as exclusionary structures. To ensure equitable access to recovery capital, communities must adopt intentional strategies that mitigate social stratification based on mental health status.
This study addresses a gap in recovery literature by using longitudinal network analysis to separate selection from influence. It provides empirical evidence that mental health status drives social connectivity in recovery settings, rather than connectedness simply improving mental health.
Introduction
Recovery from substance use disorder (SUD) is fundamentally social. Relationships shape access to support, reinforce behavioral change and influence long-term well-being. Yet despite widespread recognition that social connection matters, the mechanisms linking social ties and mental health within recovery communities remain insufficiently understood. This study uses longitudinal social network analysis to investigate these dynamics within a sober active community, a distinctive recovery context that integrates physical activity with peer support.
Social Relationships in Recovery
Social connection is a central driver of sustained recovery. Supportive relationships help individuals maintain emotional stability, reinforce abstinence norms and build what scholars term recovery capital: the social and material resources that help individuals initiate and maintain change (Best and Laudet, 2010; Cloud and Granfield, 2008). Reflecting this, national guidelines identify social support and network development as core components of effective recovery systems [Substance Abuse and Mental Health Services Administration (SAMHSA), 2024].
Community-based recovery support services have become increasingly prominent as a means of cultivating these protective social environments. Such programs offer structured, peer-driven spaces that complement clinical care and extend support beyond formal treatment (Eddie et al., 2019). Evidence consistently shows that participation in these communities reduces relapse risk, strengthens psychosocial functioning and improves treatment engagement (Hennessy, 2017).
Barriers to Social Connection in Recovery
While recovery communities are broadly protective, they are not immune to dynamics that can limit access to support. Individuals entering recovery often carry internalized stigma related to their substance use and mental health, which can inhibit social approach behaviors (Link and Phelan, 2001).
Beyond individual-level barriers, network formation processes themselves may systematically disadvantage certain members. A large body of research demonstrates that social ties tend to form between individuals who share similar characteristics, a phenomenon known as homophily (McPherson et al., 2001). Homophily can arise through multiple mechanisms: individuals may prefer interacting with similar others, shared settings may create opportunities for contact among people with common traits or social norms may channel relationships along particular lines (Kossinets and Watts, 2009). In the context of mental health, homophily processes may lead individuals with lower psychological distress to cluster together, while those with higher distress remain on the periphery, a pattern sometimes termed “homophily of well-being” (Cacioppo et al., 2009).
Social exclusion theory offers a complementary lens for understanding these dynamics. Communities naturally form boundaries, and individuals who deviate from group norms, including those displaying higher levels of distress or behavioral instability, may be inadvertently marginalized (Abrams et al., 2005). Exclusion may occur not through overt rejection but through subtler processes: distressed individuals may be perceived as less rewarding interaction partners, less capable of reciprocating support or more emotionally costly to engage with (Leary, 2007). Over time, these micro-level selection processes can produce structural isolation, leaving those with the greatest need for support with the fewest connections.
Recognizing these dynamics, scholars have called for intentional strategies to promote inclusion in network formation. Proposed approaches include structured socialization opportunities that lower barriers to initial contact, mentorship programs that pair newcomers with established members, and small-group formats that foster repeated interaction among individuals who might not otherwise connect (Valente, 2012; Hunter et al., 2019). However, empirical evidence on the effectiveness of such interventions remains limited, and questions persist about how to implement them without inadvertently stigmatizing recipients or undermining the authenticity of relationships (Corrigan, 2004; Thoits, 2011).
Consequently, while social connection is vital for recovery, structural and psychological barriers may prevent those who need support the most from accessing it. This underscores the importance of examining how social connectedness and mental well-being interact over time and whether certain individuals are systematically excluded from the networks that could support their recovery.
Mental Well-Being as a Foundation for Recovery
Mental well-being is both an outcome of recovery and a condition that sustains it. Models of complete mental health emphasize that long-term recovery depends on emotional stability, identity development and social functioning, not abstinence alone (el-Guebaly, 2012). Individuals with higher levels of positive mental health are more likely to maintain recovery over time, even when facing ongoing challenges (Iasiello et al., 2019). Understanding how mental health shifts within recovery communities is therefore essential for identifying mechanisms that promote long-term resilience.
Sober Active Communities: A Novel Recovery Model
One emerging approach to building resilient recovery networks moves beyond traditional mutual-aid meetings by leveraging shared activities and physical exertion. Sober active communities combine structured physical activity with peer support to promote social connection, identity transformation and psychological well-being (Heinrich et al., 2025). These communities create natural opportunities for relationship-building through shared challenge and accomplishment, offering members both a health-promoting activity and an accessible entry point into a recovery network (Best et al., 2016; Cloud and Granfield, 2008).
The Phoenix, a nonprofit sober active community founded in 2006, exemplifies this approach (Wyker and Hillios, 2020). Operating nationally, The Phoenix offers free fitness classes and outdoor activities to individuals with at least 48 h of sobriety. Prior research shows that Phoenix participation expands supportive networks, enhances psychological safety and is associated with lower psychological distress and greater engagement (Heinrich et al., 2025; Patterson, Francis et al., 2025; Patterson, Zhou et al., 2025). These findings align with broader evidence that social connection is a key determinant of mental health and buffers against stress. However, existing studies have not yet clarified the direction of these relationships, whether social ties improve well-being or whether individuals with better well-being are simply more likely to form ties.
Social Network Analysis as a Tool for Understanding Recovery
Addressing this question requires methods capable of capturing relational dynamics over time. Social network analysis (SNA) provides a powerful framework for examining how relationships shape behavior and well-being. By situating individuals within a network structure, SNA captures patterns of interaction that influence access to support and opportunities for change (Valente, 2010). Longitudinal network models are particularly valuable because they allow researchers to disentangle two processes that often co-occur: social selection, which reflects whether individuals choose peers based on their characteristics, and social influence, which reflects whether individuals’ behaviors or well-being shift to resemble their peers (Steglich et al., 2010). Applied to recovery communities, these models can reveal how supportive ties form, how they evolve and how they relate to changes in mental health.
The Current Study
Although emerging evidence suggests that sober active communities foster social support and promote mental well-being, most studies rely on cross-sectional or short-term designs. As a result, it remains unclear whether improvements in mental health arise because individuals form supportive ties, or whether individuals with better mental health are more likely to form those ties in the first place. Longitudinal, network-based analyses are needed to clarify these mechanisms.
This study addresses this gap by examining the co-evolution of supportive ties and psychological distress among members of The Phoenix across one year. We focus on three research questions:
What network features, such as reciprocity and transitivity, drive tie formation within The Phoenix?
Does psychological distress influence the formation of social ties (social selection), and do peers influence one another’s distress over time (social influence)?
Do newer members of The Phoenix show greater improvements in psychological distress?
Methods
Participants and procedure
Participants were members of The Phoenix CrossFit programs in Denver, Colorado and Wichita, Kansas. Prior to baseline data collection, researchers collaborated with Phoenix staff to define membership criteria. Individuals were considered members if they had attended at least one Phoenix CrossFit class in the past 30 days and participated in classes at least once per week, on average. All individuals meeting these criteria were included on site-specific rosters.
Rostered members received an email invitation describing the study with a link to an online survey. After providing electronic consent, participants completed measures assessing demographics, psychological distress and social network connections. Participants received a $40 gift card upon survey completion. The same procedures were repeated one year later.
To be included in the longitudinal analysis, participants had to appear on the roster at both waves and complete all assessments. In Denver, 12 of 15 eligible members completed both waves (80%). In Wichita, 11 of 14 eligible members completed both waves (78.6%). All procedures were approved by the institutional review board.
Measures
Social support connections. Participants completed a network generator in which they selected, from their site’s roster, all Phoenix members who “go above and beyond to support them.” They could select as many individuals as applied but were instructed not to select themselves. These directed nominations formed the basis of the network data.
Psychological distress. Psychological distress was assessed using the Kessler Psychological Distress Scale (K6), a widely used six-item measure of nonspecific distress (Kessler et al., 2002). Participants rated how often they experienced symptoms in the past 30 days on a five-point scale ranging from “none of the time” to “all of the time.” Items were summed, and to meet the analytical requirements of SIENA, which models behavioral changes as discrete micro-steps, scores were converted into six ordinal categories. Categorizing the data in this way allowed for the simultaneous examination of both individual change and potential peer influence within the model. However, we acknowledge the analytical tradeoff: compressing continuous scores into ordinal groups inherently loses data granularity and reduces the statistical sensitivity needed to detect minor, incremental shifts in psychological distress. The K6 demonstrated strong internal consistency reliability at both baseline (Cronbach’s α = 0.82) and follow-up (Cronbach’s α = 0.86).
Membership duration. Participants reported how long they had been members of The Phoenix, with response options ranging from less than six months to five or more years.
Demographics. Participants reported their gender and age.
Analytic approach
To examine the co-evolution of social ties and psychological distress, we used the Simulation Investigation for Empirical Network Analysis (SIENA) framework implemented in RSiena (Snijders et al., 2010). SIENA is designed for longitudinal network data and simultaneously estimates structural network effects and behavioral dynamics. The model treats network change as a series of small decisions in which individuals may form, maintain or dissolve ties, or adjust their behaviors, in ways that increase their utility. Parameters are estimated by simulating these micro-steps until the simulated networks match the observed data.
SIENA is particularly well suited for this study because it models network change as a sequence of micro-steps that approximate how individuals make decisions about forming, maintaining or dissolving ties. This approach is advantageous for small, bounded recovery networks, where relationships are shaped by repeated interactions and shared activities. Unlike cross-sectional network models, SIENA allows researchers to separate structural tendencies from behavioral processes, which is essential for distinguishing whether individuals choose peers based on psychological distress or whether distress levels shift in response to peers (Snijders et al., 2010).
Model specification
We estimated a pooled, two-group model using the sienaGroup function. Pooling the Denver and Wichita networks allowed us to increase statistical power while preserving the distinct boundaries of each site. This approach is recommended when networks share similar structures and measurement protocols but operate independently. Behavioral variables were modeled using ordinal categories to improve estimation stability, given the limited number of waves and the relatively small sample sizes. Convergence was evaluated using standard RSiena diagnostics, including overall maximum convergence ratios and parameter-specific t-ratios. Ratios below 0.25 indicate that simulated networks adequately reproduce observed patterns, and our model met this criterion (Ripley et al., 2021).
Model building followed a forward-selection process. We began with a comprehensive set of theoretically relevant structural and behavioral effects and retained parameters that improved model fit and aligned with the study’s research questions. The final model included three structural effects: outdegree (density), reciprocity and transitive triplets. Behavioral effects included a psychological distress alter effect to test social selection and an average alter effect to test social influence. We also included a covariate effect to assess whether shorter membership duration predicted greater improvements in psychological distress. All behavioral effects were modeled using the ordinal K6 categories. Parameters were retained based on convergence diagnostics, goodness-of-fit statistics and theoretical relevance. The final model demonstrated acceptable convergence, with a maximum convergence t-ratio of 0.16, which is within recommended thresholds (Ripley et al., 2021). See Table 1 for a summary of model parameters.
Results
Descriptive results
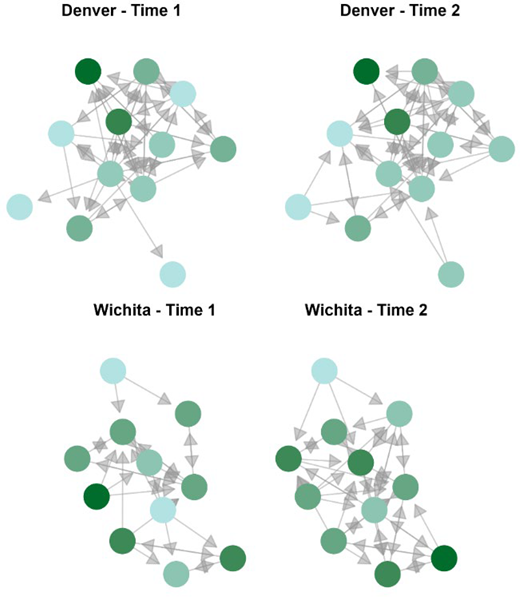
Network structure and stability. Longitudinal network data were collected from Denver (n = 12) and Wichita (n = 11). Both networks demonstrated adequate stability for SIENA estimation, with Jaccard indices of 0.63 in Denver and 0.43 in Wichita (Table 2). Connectivity increased over time in both locations. In Denver, edges rose from 52 to 57, increasing density from 0.39 to 0.43. Wichita showed a larger shift, with edges increasing from 30 to 47 and density rising from 0.27 to 0.43. Reciprocity remained high in both networks, decreasing slightly in Denver (0.77–0.68) and increasing in Wichita (0.60–0.64). Transitivity also increased in both sites, from 0.64 to 0.70 in Denver and from 0.43 to 0.65 in Wichita. See Figure 1 for a visual representation of network changes across time points.
Longitudinal attributes. Participants in Denver experienced a modest increase in in-degree, rising from an average of 4.33 to 4.75 (mean change = 0.42). Wichita participants showed a larger increase, from 2.73 to 4.27 (mean change = 1.55). Psychological distress increased slightly in both locations. Denver rose from a mean of 2.50 to 2.58 (mean change = 0.08), while Wichita increased from 2.82 to 3.09 (mean change = 0.27). Demographic characteristics were similar across sites, with average ages of 36.83 in Denver and 37.73 in Wichita, although gender composition differed. See Table 3 for a summary of attributes in both networks across time.
SIENA model results
The SIENA model identified several structural tendencies shaping tie formation within The Phoenix (Table 4). The outdegree parameter was negative and significant (estimate = −1.07, p < 0.01), indicating that members formed ties selectively rather than broadly. Reciprocity was positive and significant (estimate = 0.71, p < 0.05), suggesting that mutual support was more likely than chance. Transitive triplets were also positive and significant (estimate = 0.24, p < 0.01), reflecting a tendency toward triadic closure and cohesive clustering.
Social selection and influence. The psychological distress alter effect was negative and significant (estimate = −0.37, p < 0.05). Members with higher distress were less likely to be nominated as supportive ties, whereas those with lower distress were more likely to be selected. The average alter effect, which tests social influence, was positive but not significant (estimate = 0.41). There was no evidence that individuals adjusted their distress levels to resemble the average distress of their support network over the one-year period.
Membership duration. The effect of Phoenix membership duration on changes in psychological distress was negative but not significant (estimate = −0.59). Longer tenure at baseline did not predict greater improvements in distress within this two-wave model.
Discussion
This study examined how social networks and psychological distress co-evolved over one year among members of The Phoenix, a sober active community. Using longitudinal social network analysis, we identified structural tendencies shaping tie formation and tested whether psychological distress influenced social selection or was influenced by peers over time.
Network features driving tie formation (RQ1)
Three structural properties shaped tie formation within The Phoenix: outdegree, reciprocity and transitivity. The negative outdegree parameter reflects selective tie formation, consistent with theories suggesting that individuals have limited capacity to maintain active relationships (Dunbar, 1998). In recovery contexts, this selectivity may be intensified by the emotional demands of sobriety and the need to rebuild social identity (Best et al., 2016). As a result, participants may invest their social energy in a smaller set of trusted relationships.
Reciprocity and transitivity further characterized the network, aligning with research showing that peer support often depends on shared experiences and reciprocal exchange (Mead et al., 2001). Transitivity reflects a tendency for friends of friends to become connected, a pattern that fosters cohesion and can accelerate the development of supportive clusters (Block, 2015). For individuals rebuilding their social networks during recovery, these clustering processes may help expand recovery capital and reduce isolation (Bathish et al., 2017).
Social selection and influence (RQ2)
The SIENA model tested two processes central to understanding how mental health and social ties may be related: selection (whether individuals choose ties based on others’ characteristics) and influence (whether individuals’ well-being shifts to resemble that of their peers).
We found a significant negative alter effect for psychological distress, indicating that members were more likely to nominate peers with lower distress as supportive ties. This pattern is consistent with previous research documenting similar selection effects in recovery communities, where individuals with positive mental health indicators may be more accessible and appealing as network partners (Best and Lubman, 2017; Patterson, Zhou et al., 2025). Several mechanisms may explain this finding. First, psychological distress can reduce social motivation and visibility, making distressed individuals less likely to be perceived as available for connection (McGaffin et al., 2018). Second, individuals seeking support may, consciously or not, gravitate toward peers who appear emotionally stable and capable of reciprocating (Eddie et al., 2019; Prochnow et al., 2021). Third, distressed individuals may withdraw from social interaction or send fewer affiliative signals, reducing opportunities for tie formation (Elmer and Stadtfeld, 2020). Regardless of the specific mechanism, the practical implication is that distress may function as a structural barrier to social integration, potentially leaving those with the greatest need for support on the periphery of the network (Patterson, Zhou et al., 2025).
In contrast, the average alter effect, testing whether individuals’ distress levels converged toward those of their peers, was not statistically significant. This null finding should be interpreted with caution, as multiple factors may have contributed to our inability to detect an influence effect, and we cannot definitively distinguish among them.
First, statistical power was limited by the small network sizes (n = 12 in Denver; n = 11 in Wichita). Although convergence was acceptable and the model was estimable, SIENA models with small samples have reduced power to detect influence effects, particularly when those effects are modest in magnitude (Ripley et al., 2021). Second, the one-year interval between measurement waves may have been inappropriate for capturing peer influence on psychological distress. Influence processes such as emotional contagion or normative adjustment may unfold over weeks or months rather than years; a shorter interval might have revealed effects that our design was unable to detect (Prinstein, 2007). Third, measurement insensitivity may have obscured subtle shifts in distress. Compressing continuous K6 scores into ordinal categories for model convergence reduced variance and may have masked small but meaningful peer-driven changes in well-being. Fourth, it is possible that distress levels were genuinely stable over the observation period. Descriptive analyses revealed that 47.8% of participants reported no change in their distress quartile, and median values remained constant. If distress was stable for substantive reasons, such as participants having already achieved a recovery baseline, then there would have been limited room for peer influence to operate.
It is also possible that the null finding reflects a genuine absence of peer influence on psychological distress in this context. Unlike health behaviors such as substance use or physical activity, psychological distress may be less susceptible to peer influence processes, particularly in communities where members are at different stages of recovery and may not spend sufficient time together to shape one another’s emotional states. If this is the case, the selection effect we observed, where lower-distress individuals are preferentially chosen as ties, may be the primary mechanism linking mental health and network position in sober active communities, rather than a bidirectional process involving both selection and influence.
Given these considerations, we interpret the null influence finding conservatively: the current study did not detect evidence of peer influence on psychological distress. This may reflect methodological constraints, genuine stability in distress or an authentic absence of influence processes in this setting. Future research with larger samples, shorter or more frequent measurement intervals, and continuous outcome measures would provide a stronger test of influence processes in sober active communities.
Membership duration and psychological distress (RQ3)
Membership duration did not significantly predict improvements in psychological distress in the SIENA model. However, exploratory analyses suggested a nonlinear pattern in which the greatest improvements occurred among individuals with 1–3 years of membership. This pattern is consistent with research indicating that recovery benefits often follow a phased trajectory, with early gains emerging as individuals accumulate recovery capital and later stabilizing as they maintain progress (Kelly and Hoeppner, 2015). These findings suggest that time in the community may matter less than the quality and depth of social connections formed during that time (Berkman et al., 2000).
Limitations
Several limitations warrant consideration. First, the small network sizes constrained the complexity of model specifications, though response rates were high and convergence was acceptable. Second, data were collected at only two time points separated by one year, an interval that may be too long to detect gradual or fluctuating influence effects and that necessitated compressing continuous distress scores into ordinal categories, reducing measurement sensitivity. Third, self-reported measures may not capture moment-to-moment fluctuations in mental health. Future studies with larger networks, additional time points and more granular measurement approaches would strengthen the ability to detect peer influence and nonlinear change trajectories.
Implications for research and practice
These findings have several implications for both research and practice in recovery communities. First, our finding of selective tie formation (density) highlights the importance of fostering trust-building opportunities and promoting secure environments where individuals feel safe forming new supportive ties without risking instability (Best and Hennessy, 2022; Heinrich et al., 2025). Future research should examine whether interventions designed to lower perceived barriers to new connections, particularly for those newer to recovery, can facilitate the expansion of trustworthy, reciprocal networks (Bell et al., 2019; Di Bartolomeo and Papa, 2019; Falk and Fischbacher, 2006).
Second, our finding that psychological distress may hinder social integration suggests that practitioners should attend to whether individuals with higher levels of distress are becoming socially isolated within recovery communities (Elmer and Stadtfeld, 2020; Prochnow and Patterson, 2025). While our study did not test specific interventions, these results point to the need for future research examining whether structured approaches, such as formalized mentorship dyads or intentional small-group formats, might mitigate the tendency for high-distress members to be filtered out by the network’s natural selection dynamics (Hunter et al., 2019; Valente, 2012; Vilsaint et al., 2025). However, such approaches warrant careful implementation and evaluation, as they may carry unintended consequences. Assigned relationships could inadvertently stigmatize recipients by publicly signaling that they are struggling, potentially reinforcing internalized stigma or marking individuals as “in need of help” in ways that undermine their social standing within the community (Corrigan, 2004). Formalized pairings may also feel less authentic than organically developed ties, reducing their perceived value and emotional impact for both parties (Thoits, 2011). In addition, mentors or designated supporters may experience burden or compassion fatigue, particularly if pairings are not well-matched or adequately supported (Moll et al., 2009). Future experimental or quasi-experimental research should therefore assess not only whether structured integration approaches effectively connect at-risk individuals to social capital, but also whether they produce unintended harms – and under what conditions benefits outweigh costs.
Third, this study contributes to a larger body of work highlighting the relationship between social connectedness and mental wellbeing (McGaffin et al., 2018; Patterson, Zhou et al., 2025). Given the importance of social connectedness and support in successful recovery, and the relationship we observed between mental wellbeing and network position, mental health should remain a priority for recovery communities and other SUD treatment settings.
Finally, our findings suggest several directions for future research. As noted in the limitations, studies with additional time points and qualitative components could reveal more about how social connections and mental wellbeing co-evolve. In addition, since our findings suggests a tendency toward stable network ties and mental well-being among longer-term members of The Phoenix, future research could focus specifically on new members and how their connections and mental health adjust over time. Methodological innovations may also prove valuable; for example, natural language processing approaches have the potential to detect more nuanced and real-time mental health status, and these methods continue to evolve alongside advances in large language models (Calvo et al., 2017).
Conclusion
Social connections within The Phoenix were characterized by selective, reciprocal and transitive ties that fostered cohesion while limiting indiscriminate expansion. Members with lower psychological distress were more likely to be chosen as supportive partners, highlighting a potential gap in inclusion for individuals who may need support the most. The study did not detect evidence of peer influence on distress. This may reflect methodological constraints, including small sample sizes, a one-year measurement interval and reduced measurement sensitivity, or it may indicate that peer influence on psychological distress is limited or absent in this context. Membership duration alone did not predict improvements in mental health. These findings underscore the dual role of recovery networks as protective yet potentially exclusionary structures and highlight the importance of intentional strategies that promote trust, reciprocity, inclusion and the accumulation of recovery capital.
The authors would like to thank The Phoenix for their partnership on this project. Specifically authors want to thank Dr. Beth Collinson for serving as the connection point between the researchers and participants; Mika Mumme and Rob Baumgartner for being their contact staff for recruitment in Denver, Colorado; Cody Palmer for being their contact staff for recruitment in Wichita, Kansas; and the Phoenix members in Denver and Wichita who were willing to participate in their study.