

Integrated health and social care initiatives are increasing and health and social care systems are aiming to improve health and social outcomes in disadvantaged groups. There is a global dialogue surrounding improving services by shifting to an integrated health and social care approach. There is consensus of what is “health care”; however, the “social care” definition remains less explored. The authors describe the state of “social care” within the current integrated care literature and identify the depth of integration in current health and social care initiatives.
A narrative literature review, searching Medline, PsychINFO, CINAHL, PubMed, Scopus and Cochrane databases and grey literature (from 2016 to 2021), employing a search strategy, was conducted.
In total. 276 studies were eligible for full-text review, and 33 studies were included and categorised in types: “social care as community outreach dialogues”, “social care as addressing an ageing population”, “social care as targeting multimorbidity and corresponding social risks factors” and “social care as initiatives addressing the fragmentation of services”. Most initiatives were implemented in the United Kingdom. In total, 21 studies reported expanding integrated governance and partnerships; 27 studies reported having health and social care staff with clear integrated governance; 17 had dedicated funding and 11 used data-sharing and the integration of systems’ records.
The authors' demonstrate that social care approaches are expanding beyond the elderly, and these models have been used to respond to multimorbidity [including coronavirus disease 2019 (COVID-19)], targeting priority groups and individuals with complex presentations.
Background
The recognition of social factors impacting health outcomes has been well established (Braveman and Gottlieb, 2014; Amelung et al., 2021; Aboutanos et al., 2019). It is understood that addressing the social needs of health consumers can improve health outcomes at a population level (Amelung et al., 2021; Cartier and Gottlieb, 2020).
It has been postulated that developing systems that foster integrated health and social care (Gottlieb et al., 2017; Braveman and Gottlieb, 2014; Murphy et al., 2017) are fundamental to reducing overreliance on institutional care (e.g. hospital admissions and emergency presentations) and addressing social needs.
Historically, social care efforts have predominately focussed on pension systems, home-help and residential services for the elderly (Peck, 2001; National Academies of Sciences et al., 2020). More recently attention has been placed on social care models addressing integrated social and health-related needs (Cartier and Gottlieb, 2020; Wodchis et al., 2020).
Importantly, policies and legislative frameworks have been developed and evolved to facilitate joined-up health and social care in mature systems, including introducing new care models and accelerating take-up in local areas showing the slowest progress (House of Commons Committee of Public Accounts, 2018).
There has been an expansion of social models of care (and its evaluation) into health care systems, including routine screening for social risks, social needs assessment, integrated global health plans, care coordination, social-based interventions (e.g. social prescribing) primarily originating from the United Kingdom (UK) (Islam, 2020) and the United States of America (USA) (Gottlieb et al., 2017; Cartier and Gottlieb, 2020). However, the definition of what constitutes “social care” and how it should be systematically integrated is less well understood (Amelung et al., 2021).
Key to advancing the global dialogue is a clear definition of what the “social” aspect of integrated health and social care is (Amelung et al., 2021). Without this, there is the risk of (1) social aspects of integrated care being lost within the more dominant field of integrated (community and hospital) healthcare, (2) creating a conceptualisation of integrated health and social care that is too broad and diffuse for new audiences to grasp and (3) certain aspects of social care dominating the dialogue.
Moreover, it has been argued that social care has been consistently perceived as an add-on to health care services, which can be exacerbated by the lack of “parity of esteem” between the health and social care systems (Quilter-Pinner and Hochlaf, 2019).
One of the crucial aspects that could facilitate change in the paradigm is to develop comprehensive integrated health and social care policies at global and local levels. Wodchis et al. (2020) postulate that depth of true integration can be measured by the level of support and expansion of (1) integrated governance and partnerships; (2) integrated workforce and staffing; (3) integrated financing and payment and (4) data-sharing and use (Wodchis et al., 2020). These authors used a hybrid integrated care framework (Peter Long et al., 2017; Leijten et al., 2017; WHO, 2016) to assess the depth of integration of 30 integrated health and social care programmes in high income countries.
Against this backdrop, the severe acute respiratory syndrome COVID-19 (SARS-COV-2) pandemic reemphasised the interdependence of the health and social care sectors. Health systems have started to utilise novel approaches to address social needs of vulnerable communities worldwide (Paremoer et al., 2021; Abrams and Szefler, 2020). The pandemic has accelerated demands for information about patients’ social circumstances to assess for risks of contracting the virus and/or spread it in their community. Novel and expanded social risk screening have been conducted to alert primary care providers about patients whose social challenges put them at higher risk of COVID-19 complications (Gottlieb et al., 2021).
COVID-19 has also driven health systems to incorporate and expand the types of socio-economic risks included in social assessments, including employment, education and housing arrangements. In part, this is driven by new policies or encouragement from health care departments (Gottlieb et al., 2021). As the effects of the pandemic impact on delivery and access to health and social care, it is an appropriate time to apply lessons learnt and to re-assess and enhance efforts to strengthen, scale and sustain integrated health and social care health care (Singu et al., 2020).
Present study
Given the lack of current definition of “social care”, and the lack of clarity on the levels of true integration, a narrative review study sought to (1) describe the current state and types of “social care” within the current integrated care space and (2) assess the level of integration regarding governance and partnerships; workforce and staffing; financing and payment and data-sharing and use in recent integrated health and social care initiatives.
Methods
A narrative review, using an interdisciplinary approach, and broad scope of topics related to social care in the context of integrated health and social care was conducted.
A search of the academic databases was conducted for studies reporting on the design, implementation, effectiveness and experiences of interventions and system change models integrating health and social care for the period 2016 to 2021. This period was chosen given a higher uptake of integrated health and social care initiatives in the last 5 years.
Eligibility criteria
The following inclusion criteria were utilised:
Intervention: Integrated health care and social care interventions that were based in a primary, secondary and tertiary health care settings as well as community and placed based settings. Integrated health care settings without social care were excluded.
Study design: All published study types were included including pilot studies, case studies, randomised controlled trials (RCT), quasi RCT and non-RCT studies.
Population: Participants, defined as enrollees, clients, patients or recipients, of integrated health and social care programmes across the lifespan.
Language: English.
Search strategy
The systematic search was conducted in December 2021 by first the author (GU) using the following: Medline, PsychINFO, CINAHL, PubMed, Scopus and Cochrane and grey literature. This was completed using keyword searches, free search terms and their associated MeSH headings. MeSH headings used included “Integrated”, “Health”, “Social” and “Care”. These searches were replicated as closely as possible across the six databases.
Terms used for the search are outlined below:
 Following the identification of these articles, two reviewers (GU and FCM) independently screened all articles based on their title and abstract for inclusion based on the eligibility criteria described above. Any discrepancies between the two reviewers were revisited again by both reviewers, with a third reviewer (CHS) brought in to reach a consensus if there were still any disagreements. All articles that met our eligibility criteria were reviewed based on their full text by two reviewers (GU and FCM). Discrepancies were also discussed again by both reviewers, with a third reviewer (CHS) brought in to reach a consensus if there were still any disagreements.
Following the identification of these articles, two reviewers (GU and FCM) independently screened all articles based on their title and abstract for inclusion based on the eligibility criteria described above. Any discrepancies between the two reviewers were revisited again by both reviewers, with a third reviewer (CHS) brought in to reach a consensus if there were still any disagreements. All articles that met our eligibility criteria were reviewed based on their full text by two reviewers (GU and FCM). Discrepancies were also discussed again by both reviewers, with a third reviewer (CHS) brought in to reach a consensus if there were still any disagreements.
Data extraction
One reviewer (GU) extracted data from the included studies utilising CovidenceTM software. Data extracted included study design and location, sampling method, participants, target group, care coordination component/characteristics, health and social health components and characteristics regarding organisation/s or body supporting/leading the system integration.
Framework for analysis
We analysed the extracted data in two steps. First, we undertook an inductive interpretive analysis of the scope of activities within each reported initiatives to determine how “social care” was defined. In the second step, using a framework devised by Wodchis et al. (2020), we reviewed the extent to which each of the described initiatives were integrated beyond the life of a pilot or fixed-term programmes. The core components of this framework and description are synthetised in Table 1.
Framework by Wodchis et al. (2020)
| Category | Description |
|---|---|
| Integrated governance and partnerships | Characterised by new form of governance or new collaborative partnerships between health and social care organisations. Programmes can be also reported to have substantive changes in the governance of local health care, the extent of local partnerships required to implement the programmes or both |
| Integrated workforce and staffing | New approaches to staffing or work roles are undertaken. Expanding the roles of providers, adding new roles or finding new ways of working for existing providers. Programmes with supportive workforce or staffing policies with new local efforts to have health and social care providers work together, with or without adding staffing roles or the creation of multidisciplinary team-based care |
| Integrated financing and payment | Identified financing and payment policy changes as essential supports. This can involve new budgets created to cover the full cost of all health and social care services for the target populations. Aggregated or bundled budgets, new envelopes of funding for central programmes and sophisticated risk-sharing contract with delivery organisations and the insurance companies can also be mapped |
| Data-sharing and use | New approaches to data or information technology. Share patient information to have access to the clinical records of another group. Other forms could include staff sharing information about patients across providers. Secondary uses of data include programmes creating standard reporting on programme statistics (such as number of patients), which mirror existing approaches to data monitoring or programmes using rigorous third-party external (often university-based) evaluators to manage data and report on the programme outcomes |
Results
A preferred reporting items for systematic reviews and meta-analyses (PRISMA) flowchart is provided as Figure 1. Of the six databases searched up and until the 30th of November 2021, our searches yielded 4,125 studies. Based on title and abstract screening, 276 studies were eligible for full-text review, with 33 of these studies being included in the final narrative review.
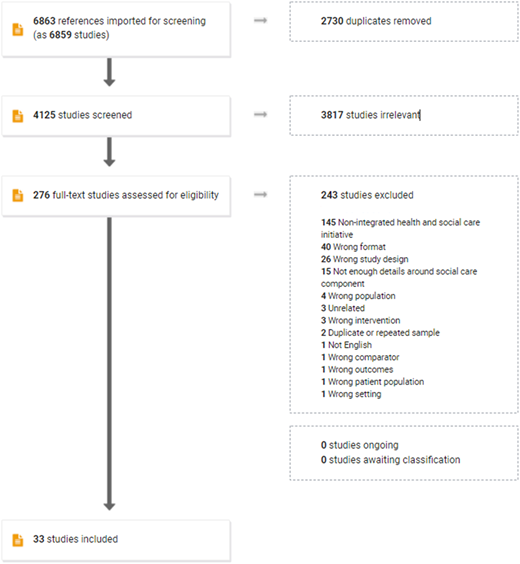
Table 2 provides details on each of the selected studies, country, including aims, study design, type of participants, sample sizes, sampling and relevance (target population). The top 3 countries reporting health and social care initiatives in the literature are the UK (n = 13), followed by the USA (n = 7) and the Netherlands (n = 4). Studies focussed on providing social care for older adults (n = 13) (Terracciano et al., 2021; Aredes et al., 2021; Pruitt et al., 2018; Perman et al., 2021; Mateo-Abad et al., 2020; Vestjens et al., 2019; Spoorenberg et al., 2019; Elston et al., 2019; Wong et al., 2020; Sadarangani et al., 2019; Tong et al., 2020; Doheny et al., 2020; Janse et al., 2016), followed by initiatives targeting social care for multimorbidity (n = 14) (Melvin and Gipson, 2019; Collins et al., 2017; Moretti, 2017; Davenport, 2021; Zarnegar et al., 2017; Eastwood et al., 2019; Talbot et al., 2020; de Vries McClintock et al., 2016; Ismail et al., 2020; White et al., 2021) and corresponding social needs (Aboutanos et al., 2019; Cammy, 2017; Van Dijk et al., 2016; Pauley et al., 2016), initiatives addressing fragmentation of systems more broadly (n = 3) (Bussu and Marshall, 2020; Murphy et al., 2017; Alexander et al., 2018) and initiatives aimed at community outreach in the context of integrated care (n = 3) (Moon et al., 2021; Chng et al., 2021; Sohanpal et al., 2017).
Descriptive of selected health and social care initiatives
| Authors and year | Title | Country | Aim of study | Study design | Participants | Total number of participants | Target population |
|---|---|---|---|---|---|---|---|
| Aboutanos et al. (2019) | Critical call for hospital-based domestic violence intervention: The Davis Challenge | United States | Describe the 10-year initial development, sustainability, and growth of a hospital-based intimate partner violence (IPV) intervention programme at a Level I Trauma Centre and provide descriptive statistics on the process, outcome, and impact | Non-randomised experimental study | Patients and clinicians | n = 799 patients n = 1,130 staff and service providers | Patients experiencing domestic violence |
| Alexander et al. (2018) | A before-and-after study of integrated training sessions for children’s health and care services | UK | Evaluate the efficacy of an intersectoral educational intervention across children services for improving participants’ knowledge of local services and improving participants’ joint working status (including communication, navigation and confidence in collaboration) | Non-randomised experimental study | Clinicians | n = 202 service providers | Children and families who live in disadvantaged communities |
| Aredes et al. (2021) | Integrated Care in the Community: The Case of the Programa Maior Cuidado (PCM) (Older Adult Care Programme) in Belo Horizonte-Minas Gerais, BRA | Brasil | Evaluation of the Older Adult Care Programme and examine the processes that led to the establishment of programme | Mixed-methods evaluation study | Patients and clinicians | n = 1980 patients n = 9 PMC health districts’ focus groups | Ageing population |
| Bussu et al. (2020) | Integrated care case (Dis)integrated care? lessons from east London | UK | Analyse of the perceptions of health and social care professionals working within acute and community settings in the three East London municipalities and their experience of integrated care | Qualitative evaluation study | Clinicians | Locality A: n = 36 interviews (including 1 group interview with two participants) Locality B: n = 22 interviews (including 1 group interviews with 3 participants) Locality C: n = 23 interviews (including 3 group interviews, two including with 2 participants and one including 3 participants) | Patients using primary care |
| Cammy et al. (2017) | Developing a Palliative Radiation Oncology Service Line: The Integration of Advance Care Planning in Subspecialty Oncologic Care | United States | Examine a new multidisciplinary model of care in palliative radiation oncology with contributions of the palliative radiation oncology social worker | Descriptive study | Patients | n = 26 patients | Palliative care patients |
| Chng et al. (2021) | Implementing social prescribing in primary care in areas of high socio-economic deprivation: process evaluation of the “Deep End” community links worker programme (LWP) | UK | Evaluate the implementation of the link worker programme in the seven intervention practices and explore the extent to which the programme was integrated into routine practice | Qualitative evaluation study | Clinicians | n = 31 service providers and key stakeholders (focus groups) n = 57 service providers (online survey) n = 14 services providers (depth interview with Lead GPs and community link workers) n = 19 Lead GPs, community link workers and practice managers (end-of-evaluation interviews) | Adults with multimorbidity |
| Collins et al. (2017) | Integrated human immunodeficiency virus care and service engagement amongst people living with HIV (PLHIV) who use drugs in a setting with a community-wide treatment as prevention initiative: A qualitative study in Vancouver, Canada | Canada | Generate insights into how the Dr. Peter Centre s (DPC) integrated services model influences access to, and retention in, HIV care amongst structurally vulnerable PLHIV who use drugs | Qualitative evaluation study | Patients | n = 30 patients | Patients suffering from human immunodeficiency virus and substance use problems |
| Davenport et al. (2021) | Impact of occupational therapy in an integrated adult social care service: Audit of Therapy Outcome Measure (TOM) Findings | UK | Demonstrate occupational therapy outcomes in adult social care through use of the Therapy Outcome Measure findings | Cross-sectional study | Patients | n = 70 patients | Adults (wide range) with chronic conditions which reduces occupational performance |
| De Vries McClintock et al. (2016) | Diabetes and depression care: A randomised controlled pilot trial | United States | Carry out a randomised controlled pilot trial to test the effectiveness of an integrated intervention for Type 2 diabetes mellitus (T2DM) and depression incorporating patients’ financial, social and emotional needs using patient prioritized planning (enhanced intervention) versus an integrated intervention alone (basic intervention) | Randomised controlled trial | Patients | n = 78 patients | Adults with multimorbidity |
| Doheny et al. (2020) | Impact of integrated care on trends in the rate of emergency department visits amongst older persons in Stockholm County: an interrupted time series analysis | Sweden | Investigate the potential association between the implementation of an integrated care (IC) system and the changes in the trends of ED visits in Norrtälje | Quasi-experimental cross-sectional study (interrupted time analysis) | Patients | Population-based registers covering the entire population of Stockholm County from Region Stockholm Healthcare Administrative Database | Ageing population |
| Eastwood et al. (2020) | Designing Initiatives for Vulnerable Families: From Theory to Design in Sydney, Australia | Australia | Evaluate the Healthy Homes and Neighbourhoods (HHAN) initiative, focussing on the care coordination component of the programme, using a critical realist case study approach | Pilot realist evaluation study | Patients and clinicians | n = 12 patients n = 21 staff and services providers (NGOs, GPs, NSW Department of Education, Family and Children Services) | Children and families who live in disadvantaged communities |
| Elston et al. (2019) | Improving Hospital at Home for frail older people: insights from a quality improvement project to achieve change across regional health and social care sectors | UK | Evaluate the impact of a holistic link-workers on service users’ well-being, activation and frailty, and their use of health and social care services and the associated costs | Economic evaluation | Patients | n = 86 patients | Ageing population |
| Ismail et al. (2020) | A pilot study of an integrated mental health, social and medical model for diabetes care in an inner-city setting: Three Dimensions for Diabetes (3DFD) | UK | Test whether 3DFD was associated with greater change in glycaemic control, other diabetes-related biomedical outcomes and in healthcare | Randomised controlled trial | Patients | n = 292 control group n = 277 intervention group | Adults with multimorbidity |
| Janse et al. (2016) | Do integrated care structures foster processes of integration? A quasi-experimental study in frail elderly care from the professional perspective | Netherlands | Measure integration processes in the delivery of integrated care as perceived by professionals | Quasi-experimental study with a control group | Clinicians | n = 120 control group n = 60 intervention group | Ageing population |
| Mateo-Abad et al. (2020) | Impact of the CareWell integrated care model for older patients with multimorbidity: a quasi-experimental controlled study in the Basque Country | Spain | Evaluate, in the Basque Country, the impact of the CareWell integrated care model for older patients with multimorbidity, using quantitative and qualitative techniques | Quasi-experimental controlled study | Patients | n = 99 control group n = 101 intervention group | Ageing population |
| Melvin et al. (2019) | The Open Arms Healthcare Centre’s Integrated Human Immunodeficiency Virus Care Services Model | United States | To determine if an integrated model of human immunodeficiency virus care resulted in increased linkage to care, increased treatment adherence rates, increased retention rates and improved viral load suppression | Quasi-experimental, cross-sectional research design | Patients | n = 231 patients | Patients suffering from human immunodeficiency virus |
| Moon et al. (2021) | Addressing Emotional Wellness During the COVID-19 Pandemic: the Role of Promotores in Delivering Integrated Mental Health Care and Social Services | United States | Investigate the role of promotores de salud (community health workers) in providing community-led and integrated mental health care and social services in response to the COVID-19 pandemic | Pilot evaluation study (retrospectively) | Patients | n = 776 patients (demographic analysis) n = 57 patients enrolled in the Emotional Wellness programme | Working-class Black and Latino communities |
| Moretti et al. (2017) | From the hospital towards social reintegration: the support path for people with severe acquired brain injury (ABI) and their families | Italy | Analyse the elements of the design of a programme tailored for patients with severe acquired brain injury | Descriptive study | Patients | n = 18 patients | Patients with severe acquired brain injury |
| Murphy et al. (2017) | Health benefits for health and social care clients attending an Integrated Health and Social Care day unit (IHSCDU): a before-and-after pilot study with a comparator group | UK | Identify whether attendance at the unit affected selected outcomes of functional mobility, number of prescribed medications and physical and psychological well-being | Evaluation study with a pre and post design | Patients | n = 33 control group (comparator) n = 30 intervention group | All age groups, individuals experiencing multimorbidity |
| Pauley et al. (2016) | Evaluation of an Integrated Cluster Care and Supportive Housing Model for Unstably Housed Persons Using the Shelter System | Canada | Evaluate the feasibility of an integrated cluster care and supportive housing model | Pilot evaluation study | Patients and clinicians | n = 212 patients’ usage data (retrospective) n = 31 (sub sample) patients for prospective analysis of goal achievement and satisfaction with the programme n = 20 staff members | Homeless, underhoused, and marginalised individuals with difficulties in accessing health and support services |
| Perman et al. (2021) | Effectiveness of a health and social care integration programme for home-dwelling frail older persons in Argentina | Argentina | Evaluate the effectiveness of a pilot on health and social integration aimed at reducing hospital admission rate of the participants compared to the current best standard of care | Quasi-experimental study with a concurrent control group | Patients | n = 121 control group n = 121 intervention group | Ageing population |
| Pruitt et al. (2018) | Expenditure Reductions Associated with a Social Service Referral Program | United States | Examine the association between met social needs in a social referral programme | Economic evaluation study | Patients | n = 1,521 patients (all social needs met) n = 1,197 patients (no social needs met) | Ageing population |
| Sadarangani et al. (2019) | A Mixed-Methods Evaluation of a Nurse-Led Community-Based Health Home (CBHH) for Ethnically Diverse Older Adults With Multimorbidity in the Adult Day Health Setting | United States | Evaluate outcomes associated with the CBHH model, changes in social and emotional aspects of health after 12 months in the programme and explore the perspectives of key stakeholders | Exploratory study with a sequential mixed-methods design | Patients and clinicians | n = 126 patients (EMRs*) n = 40 staff, services providers and caregivers | Ageing population |
| Sohanpal et al. (2017) | The impact of a social prescribing service on patients in primary care: a mixed-methods evaluation | UK | Present data about the effect of the service on the people referred and the implementation of the service from a patient perspective | Controlled evaluation study | Patients | n = 302 control group n = 184 intervention group | Patients in primary care |
| Spoorenberg (2019) | Health-Related Problems and Changes After 1 Year as Assessed With the Geriatric ICF Core Set (GeriatrICS) in Community-Living Older Adults Who Are Frail Receiving Person-Centred and Integrated Care From Embrace | Netherlands | Assess the prevalence and severity of health-related problems and the change after receiving individual care and support from Embrace programme | Evaluation study with a pre and post design | Patients | n = 136 patients | Ageing population |
| Talbot et al. (2020) | Delivering an integrated Adolescent Multi-Agency Specialist Service to families with adolescents at risk of care: Outcomes and learning from the first ten years | UK | Describe the Adolescent Multi-Agency Specialist Service (AMASS) approach to adolescent edge of care which aims to attend to the needs of both the family and their allocated social worker | Pilot evaluation study with a pre and post design | Patients | n = 153 families | Young people at risks of entering foster care systems |
| Terracciano et al. (2021) | The effect of community nurse on mortality and hospitalisation in a group of over-75 older adults: a nested case-control study | Italy | Assess the causal association of an integrated social and health programme including social intervention with the community nurse activity | Nested case-control study | Patients | n = 1,031 patients | Ageing population |
| Tong et al. (2020) | Effect of an integrated care model for pre-frail and frail older people living in community | China | Examine the effectiveness of an integrated care model supported by frailty assessment, personalised care plans and coordinated care services as arranged by community centres for older people in pre-frail and frail condition | Controlled, pair-matched evaluation study with a pre and post design | Patients | n = 270 control group n = 183 intervention group | Ageing population |
| VanDijk et al. (2016) | Effects of an integrated neighbourhood approach on older people’s (health-related) quality of life and well-being | Netherlands | Evaluate the effects of integrated neighbourhood approach on older people’s (health-related) quality of life and well-being life and well-being | Quasi-experimental study with a pre, post and follow-up design | Patients | n = 186 control group n = 186 intention to treat n = 186 intervention group | Community-dwelling older people |
| Vestjens et al. (2019) | Cost-effectiveness of a proactive, integrated primary care approach for community-dwelling frail older persons | Netherlands | Evaluated the Finding and Follow-up of Frail older persons (FFF) approach, which aims to maintain or improve older people’s well-being and is implemented by part of the Dutch general practitioners (GPs) | Matched quasi-experimental design with one pre and post design | Patients | n = 232 control group n = 232 intervention group | Ageing population |
| White et al. (2021) | Bridging the gap: A new integrated early intervention service for young people with complex mental health issues | Australia | Describe the young people’s pathway through headspace Early Intervention Teams (hEITs) hEIT including clinical outcomes, services delivered and experience of service. viability, development and retainment of the hEIT service and similar models going forward | A retrospective study of file audit of the electronic medical records | Patients | n = 26 patients | Young population at risk of developing mental health problems |
| Wong et al. (2020) | Effectiveness of a health-social partnership programme for discharged non-frail older adults: a pilot study | China | To test a community-based health-social partnership programme to support non-frail older adults living with optimum quality of life in their own environment after hospital discharge | Randomised controlled trial | Patients | n = 38 control group n = 27 intervention group | Ageing population |
| Zarnegar et al. (2017) | A clinical evaluation of a community-based rehabilitation and social intervention programme for patients with chronic pain with associated multi-morbidity | UK | Evaluate a community-based rehabilitation and social intervention programme which employs the components of the King’s Fund “House of Care” model | Quantitative evaluation study with a pre and post design | Patients | n = 24 patients | Patients with chronic pain and multimorbidity |
Aim 2. what is the current state and types of “social care” within the current integrated care space?
Social care was defined by four main types (Figure 2), including (1) community outreach dialogues, (2) supporting ageing populations, (3) targeting multimorbidity and corresponding social factors and (4) addressing fragmentation of services.
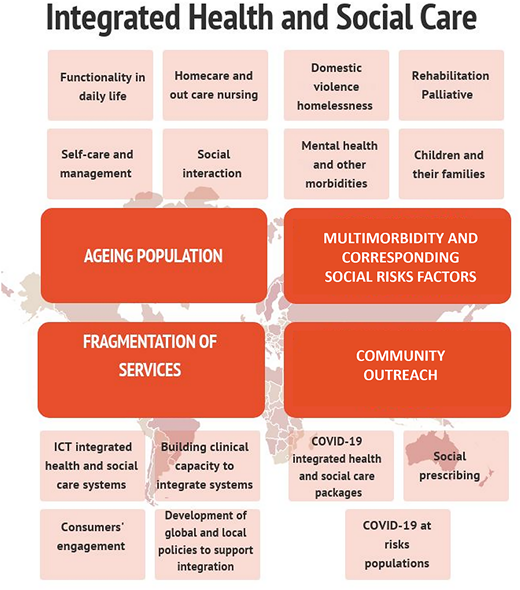
“Social care as community outreach dialogues” involves innovative and emerging social care strategies seeking to address service gaps and past failures when integrating social care enhanced by a dynamic COVID-19 pandemic backdrop.
“Social care as supporting ageing population” is comprised by all the initiatives that focuses on improving health and social outcomes for the elderly (frail, non-frail and dwelling).
“Social care targeting multimorbidity and corresponding social factors” involves initiatives aimed at addressing the needs of varied cohorts with complex needs, including pain management and functionality, acquired brain injury and occupational health, end- of-life social needs, domestic violence (DV), youth and mental health needs amongst others.
The next type is comprised of initiatives addressing fragmentation of services, creating a bridge between health and social care systems. This is primarily approached by exploring global barriers and facilitators of integration at a system level (e.g. evaluation of integrated information technology systems for health and social care).
All initiatives described in the literature (n = 33) had a care coordination component (a dedicated position assigned with the role of coordinating all the aspects of social and health care).
Social care as community outreach
There were three initiatives under this category. There is no doubt that COVID-19 has accelerated the development of social systems and care to address social needs and risks. In 2021, an initiative was implemented to provide community-led and -integrated mental health care and social services in response to the COVID-19 pandemic in Latino communities utilising promotores de salud (community health workers) (Moon et al., 2021). Two other initiatives focussed on social prescribing by utilising community link workers to support vulnerable individuals experiencing social and health multimorbidity in the UK (Chng et al., 2021; Sohanpal et al., 2017). Interestingly, two of the initiatives described in this category emerged in response to accelerated awareness, during the COVID-19 pandemic, of the need to reach and meet the social needs of marginalised populations.
Social care as supporting ageing populations
Selected initiatives that provided health and social care initiatives to older adults (n = 13), focussed on supporting specific needs of the elderly via face to face and/or home based and/or outreach and/or phone based. Key characteristics of “social care” within this category of initiatives include social care assessments and personalised plans to target older adults' social needs. Six initiatives (Perman et al., 2021; Terracciano et al., 2021; Aredes et al., 2021; Vestjens et al., 2019; Doheny et al., 2020; Janse et al., 2016) provided practical support (e.g. paid carers, home carers, home nurse and domestic helpers) and home space adaptation as part of their social care package. One initiative (Pruitt et al., 2018) provided telephone referral services (only) staffed with representatives who have personal experiences with the social service system. Six initiatives (Mateo-Abad et al., 2020; Spoorenberg et al., 2019; Elston et al., 2019; Wong et al., 2020; Sadarangani et al., 2019; Tong et al., 2020) included an intensive service coordination component (outsourcing or establishing connections with existing services) along with capacity building to increase older adults' capability to manage their conditions.
Social care targeting multimorbidity and corresponding social risks factors
In total, 14 selected initiatives aimed at targeting health and social multimorbidity and corresponding risk factors (n = 14). Two initiatives (Melvin and Gipson, 2019; Collins et al., 2017) addressed the health and social needs of (1) people living with HIV. Both provided social care referrals to services (transportation, emergency food assistance, housing and legal service) and delivery of social programmes (music, art and recreational ousting) and care coordination, although only one of them provided in-house low-threshold nursing care services (e.g. health assessments, medication assistance, support and symptom management) (Collins et al., 2017).
Three initiatives focussed on integrated health and social care for (2) people in rehabilitation (Moretti, 2017; Davenport, 2021; Zarnegar et al., 2017). An initiative to address chronic conditions and reduce occupational performance in adults was undertaken with the assistance of occupational therapists (Davenport, 2021); an initiative that used social workers to accompany people with acute brain injury (ABI) and their families for six months to conduct a support path, from hospital discharge to home care and social reintegration (Moretti, 2017) and an initiative that focussed on pain management, that included artistic, musical and horticultural activities, visits and outings as well as supporting social referrals and applications (e.g. for disability benefits for pensions or looking for employment) (Zarnegar et al., 2017).
There were two initiatives that developed integrated social care for (3) families and children experiencing vulnerability and disadvantages (Eastwood et al., 2019; Talbot et al., 2020). Three initiatives provided integrated health and social care for (4) people with mental health and other co-occurring conditions (de Vries McClintock et al., 2016; Ismail et al., 2020; White et al., 2021), utilising a combination of interventions delivered by health and non-health professionals to support adherence to treatment and to assist with application to receive social welfare. Social care initiatives that targeted (5) social risks factors such as intimate partner violence (Aboutanos et al., 2019) and initiatives targeting housing instability (Van Dijk et al., 2016; Pauley et al., 2016) have also been implemented. Finally, one integrated social care focussed on (6) end-of-life care for terminal patients and their families led by social workers (Cammy, 2017).
Social care as patching fragmentation of systems
Of the 33 initiatives selected, 3 aimed at improving fragmentation in health and social care systems (Bussu and Marshall, 2020; Murphy et al., 2017; Alexander et al., 2018). These included a service integration training package targeting clinicians’ literacy around social services when conducting early interventions with children and their families (Alexander et al., 2018); an initiative that identified collaborative approaches and services for all sectors of society and age groups (Murphy et al., 2017) in the context of integrated care in the UK; and a novel system introducing care navigators who support complex adults and help them navigate the health and social care system (Bussu and Marshall, 2020).
Aim 2. What is the level of integration regarding governance and partnerships, workforce and staffing, financing and payment and data-sharing use in the context of integrated health and social care?
We reviewed the literature for evidence that health and social care are being integrated beyond the point of pilots or time-limited programmes and to what extend the initiatives are fostering joint governance and decision-making, integrated workforce and staffing, integrated financing systems and data-sharing and use. Supplementary File outlines the data extracted by category for each initiative in detail.
Of the 33 initiatives reported in the reviewed literature, 11 were jointly led, by either a combination of tertiary education (universities and research centres) organisations and primary health networks or public health systems (hospitals and community/day health centres) and/or non-for-profit organisations (Terracciano et al., 2021; Moretti, 2017; Bussu and Marshall, 2020; Van Dijk et al., 2016; Spoorenberg et al., 2019; Ismail et al., 2020; White et al., 2021; Aboutanos et al., 2019; Zarnegar et al., 2017; Sohanpal et al., 2017; Alexander et al., 2018). In total, 20 initiatives were led by primary health network or hospital systems (Aredes et al., 2021; Pruitt et al., 2018; Collins et al., 2017; Davenport, 2021; Perman et al., 2021; Moon et al., 2021; Mateo-Abad et al., 2020; Eastwood et al., 2020; de Vries McClintock et al., 2016; Talbot et al., 2020; Vestjens et al., 2019; Elston et al., 2019; Melvin and Gipson, 2019; Wong et al., 2020; Sadarangani et al., 2019; Tong et al., 2020; Doheny et al., 2020; Chng et al., 2021; Janse et al., 2016; Murphy et al., 2017), and only one initiative did not report a leading organisation/s (Pauley et al., 2016).
Integrated governance and partnerships
In total, 21 initiatives reported supporting and expanding integrated governance and partnerships by either creating professional networks with experts from other organisations or development of steering and advisory committees (Aredes et al., 2021; Collins et al., 2017; Cammy, 2017; Moretti, 2017; Bussu and Marshall, 2020; Van Dijk et al., 2016; Moon et al., 2021; Mateo-Abad et al., 2020; Eastwood et al., 2020; Talbot et al., 2020; Vestjens et al., 2019; Elston et al., 2019; Wong et al., 2020; Sadarangani et al., 2019; Doheny et al., 2020; White et al., 2021; Aboutanos et al., 2019; Janse et al., 2016; Zarnegar et al., 2017; Murphy et al., 2017; Alexander et al., 2018).
Integrated health and social care roles
In total, 27 initiatives reporting having health and social care staff integrated in practice, with a strong role description and mapping, along with clear integrated governance (Aredes et al., 2021; Terracciano et al., 2021; Pruitt et al., 2018; Cammy, 2017; Moretti, 2017; Bussu and Marshall, 2020; Perman et al., 2021; Pauley et al., 2016; Moon et al., 2021; Mateo-Abad et al., 2020; Eastwood et al., 2020; Talbot et al., 2020; Vestjens et al., 2019; Spoorenberg et al., 2019; Elston et al., 2019; Ismail et al., 2020; Wong et al., 2020; Sadarangani et al., 2019; Tong et al., 2020; Doheny et al., 2020; White et al., 2021; Aboutanos et al., 2019; Chng et al., 2021; Janse et al., 2016; Murphy et al., 2017; Sohanpal et al., 2017; Alexander et al., 2018).
Integrated financing systems
In total, 17 initiatives were designed with dedicated and sustainable funding beyond the scope of their research (Aredes et al., 2021; Bussu and Marshall, 2020; Davenport, 2021; Perman et al., 2021; Van Dijk et al., 2016; Moon et al., 2021; Eastwood et al., 2020; Talbot et al., 2020; Elston et al., 2019; Ismail et al., 2020; Sadarangani et al., 2019; Doheny et al., 2020; White et al., 2021; Chng et al., 2021; Janse et al., 2016; Aboutanos et al., 2019; Mateo-Abad et al., 2020). This was primarily sourced from health systems with ongoing service funding.
Data-sharing and use
In addition, only 11 out of 33 initiatives reported the use of data-sharing and the integration of health and social records as part of their scope of practice (Pruitt et al., 2018; Cammy, 2017; Davenport, 2021; Mateo-Abad et al., 2020; Spoorenberg et al., 2019; Elston et al., 2019; Melvin and Gipson, 2019; Sadarangani et al., 2019; Doheny et al., 2020; White et al., 2021; Aboutanos et al., 2019).
Discussion
We sought to undertake a narrative review of recent literature (2016–2021) to explore current and evolving definitions, dialogues and novel approaches to social care in the context of integrated health and social care. Our review identified 33 integrated health and social initiatives and mapped four types: social care as community outreach dialogues, social care for supporting ageing population, social care targeting multimorbidity and corresponding social risks factors and social care as patching fragmentation of systems and fragmentation of systems. The UK is still leading the development and reporting of national policies and the implementation and evaluation of integrated health and social care initiatives, which are in line with previous reports (Amelung et al., 2021). This suggests that the generation of integrated care policies (dating back the 2000) in the UK has had ripple effects that are now evidence in funding opportunities and service delivery (Amelung et al., 2021) both of which are crucial pillars for full integration of health and social care.
Whilst the most common conceptualisations of integrated health and social care is still manifested in services and programmes for older adults, there is an emerging and significant trend of similar approaches used to address social and health multimorbidity and other social risks factors targeted at vulnerable groups beyond the elderly.
Importantly, the literature we reviewed showed several recent innovations in integrating health and social care. We found integrated health and social care responses to COVID-19 are emerging, primarily in the USA and the UK in the past year and that these are innovative not only in terms of breadth and definition of social care, but also in scale, funding and governance.
Another key innovation is the introduction of the concept of “social prescribing” as a formal service provision deliverable (using service designs and methods taken from “medical prescribing”) included in health plans for consumers (and carers) which also gained traction in 2020 and 2021 (Chng et al., 2021; Sohanpal et al., 2017). This demonstrates that dialogues and understanding around social care has certainly shifted and is now evolving into a more discussed, established and recognised as valid “model of care” (Amelung et al., 2021).
Moreover, health and social care systems have now started to explore the “bigger picture” and dive and explore “why” are the systems fragmented and “how” can this be addressed, considering the perspectives of medical stuff, clinicians, frontline social workers, decision and policies makers, consumers and carers.
Unfortunately, our results indicated that only five initiatives demonstrated “full integration” by reporting “supportive and expanding integrated governance and partnerships”, “integrated workforce and staffing”, “integrated financing and payment” and “integrated data-sharing and use”. Of note, is that data-sharing is still uncommon and the least developed strategy in the reviewed initiatives. This is a recurrent challenge many systems have faced both between sectors (e.g. social vs health care systems) and intra-sector (e.g. within the health system) (Wodchis et al., 2020). Future directions should include the development of global and local policies that foster the integration of health and social care data-sharing, along with dedicated funding to support the development of information technology (IT) systems, IT staff and a dedicated unit that can support access to these data not only for internal quality improvement, but also for advancing knowledge through research whilst ensuring the confidentially of consumers (Wodchis et al., 2020).
Several limitations of this study must be noted. This study utilised only studies written in English language and consequently may have missed health and social care initiatives conducted (and written) in non-English speaking countries and in particular low- and middle-income countries. In addition, this review did not assess the studies using a quality assessment approach (sampling, quality of instruments and research procedures) mainly because our primary goal was to map “definitions of social care”, and its evolution overtime, rather than critically analyse their effectiveness.
Strength of this study includes the use of multiple reviewers for article screening and selection, and the use of an extraction tool, in an attempt to conduct a review with a more systematic approach. In addition, this review also provides with an understanding on how well these initiatives are integrating and fostering systems and that enhance integrated health and social care which is novel.
Conclusion
Social care approaches are expanding beyond assisting the elderly, and these models have been used to outreach vulnerable communities, address social and health system fragmentation and to respond to social and health multimorbidity and other social risks factors. The UK, through their mature policy framework, is delivering and leading most of the published work in integrated health and social care initiatives worldwide.
Integrated governance and partnership and health and social care staff integrated were the more used components in the initiatives reviewed. Structures to achieve full integration, including global and policy generation are still needed, and are particularly essential to support sustainable integrated financing and payments and integrated data-sharing amount multidisciplinary teams.
Funding: The first author (GU) is funded by a National Health Medical Research Centre Integrated Health and Social Health Centre for Research Excellence (No: APP1198477). JE is the Principal Chief Investigator of this grant. CHS, JG and PH are also Chief Investigators on this grant
Research ethics approval and consent to participate: This is a scoping review of literature available and retrieved from scientific databases and as such patients' involvement was not sought.
Availability of data and materials: Data and materials used during the present study are available upon reasonable request from the corresponding author.
Consent for publication: Not applicable.
Authors’ contributions: GU, CHS, JG, JE, SW, KO, CM and PH conceived and designed the study as well as the search terms. GU and FCM screened the studies for inclusion and exclusion and GU was responsible for the data extraction, with assistance from CHS. GU and TF conducted the data analyses. GU and CM draughted the manuscript. All authors made critical revisions, read and approved the final manuscript.
References
Supplementary File
Social care scopes and integration
| Authors and year | Care | Social care | Health care | Organisation/s or body supporting/leading the system integration | Mode | By whom | Supporting and expanding integrated governance and partnerships | Integrated staff and workforce | Integrated financing system | Data sharing and use of integrated records |
|---|---|---|---|---|---|---|---|---|---|---|
About anoset al.2019 | Yes | Voluntary, trauma-informed services offered are the following: (1) safety planning, including assistance in getting a protective order if requested; (2)short-term supportive counselling, referrals, and accompaniment to service providers and the legal system; (3) coordination of care between law enforcement, courts, sexual, and DV pro-grams, legal aid, and other community-based resources; (4) se-cure shelter with temporary lodging for patients and their families when in Richmond for medical treatment; (5) follow-up services, as requested/needed; and (6) crisis funds for patient needs, such as for transportation Project Empower also connect IPV patients with interdisciplinary services already offered by VCU health system including insurance or financial assistance for health care, mental health services, an addiction clinic, and obstetrician-gynaecologist care. Apart from inpatient screening, intervention, and referral, the staff work to build report and foster a sustained relationship post-discharge until the patients’ needs are met, or they no longer wish to continue services. | ED and trauma units to other in-hospital units and clinics including women health and obstetrics. | Virginia Commonwealth University (VCU)Level I trauma center has developed a multitier inters for VCU’s hospital-based injury and violence prevention programs (IVPP), historically focusing on youth violence, bums, head trauma, and distracted driving. Hospital wide adopted intervention | Face-to-face. | IPV program coordinator, lived experience program peer advocate, and Master of Social Work interns from VCU Health. | There is a partnership between VCU Sexual Assault Response Team, the Richmond Fatality Review Team, the neighboring county strangulation workgroups, and is actively involved in the Virginia Sexual and Domestic Violence Action Alliance and other statewide groups | 1130 clinical providers were trained for IPV screening and referral | Funded by local foundations grants and a Victim of Crime Act (VOCA) grant, Project Empower addresses the immediate need of IPV patients, but is limited in its resources for long-term follow-up and comprehensive community wrap around approaches | An integrated hospital EMR-IVPP Redcap database was created |
Alexanderet al. 2018 | Yes | Service integration initiative: The workshops to | Not applicable | The programme was facilitated by | Not applicable | Not applicable | The program brought | The program brought multidisciplinary teams | NR* | NR* |
clinicians covered aspect of early help, communication, resources and building capacity. Early help is defined as the principle of providing at an early point, support to children, young people and families to maximise their life and prevent other acute problems. The training focused on improving literacy around social services amongst clinicians as well as improving ability and confidence when navigating services. | the Early Help Partnership, an organisation that advises schools on statutory responsibilities regarding safeguarding and providing early support to children and families. The policies supporting this program is the Collaboration for Integrated Care and Support and Making Every Contact Count | multidisciplinar) teams together when delivering the intervention | together when delivering the intervention | |||||||
Aredes et al. 2021 | Yes | Social Assistance Reference Centre offers a wide range of services for people of all ages, with a particular emphasis on protecting and strengthening relationships between family members and guaranteeing human rights. It offers practical support by assigning home paid carers | 'Sistema Único de Saúde' (SUS) Health Centre offers comprehensive set of primary health care services to defined communities | Belo Horizontes municipal departments of health and social assistance | National coordination and local hubs for community engagement. Local hubs known as Social Assistance Reference Centres. | Family Health Teams (ESF) are responsible for referral, coordinating different SUS health services and operating as a bridge between the health system and local communities | A partnership between Belo Horizonte municipal departments of health and social assistance. Carers are hired through a contract between the municipality and governmental Civil Society Organisation (Organiza da Sociedade Civil OSC in Portuguese) | PMC management is intersectoral, with joint oversight at the central level of the Secretariats of Health and Social Assistance, and the local level through joint activities involving the CS (Centro de Salud) and CRAS teams (Centro de Referencia Social). Each CRAS has staff members with specific responsibility for PMC. At the central level, programme supervisors have overall responsibility for the management of caregivers and for care quality assurance. At the local level, PMC is supported by a close collaboration between families, health professionals, social assistance professionals and PMC carers | The finance system combines Department of Health and Social Assistance funding schemes. Social Assistance folly fonds the carers | There were gaps in the PMC data systems operated by both the departments of Health and Social Assistance, and they were mutually incompatible, thus preventing data sharing |
Bussuet al.2020 | Yes | Care navigatore were introduced. These are non-clinicians who support complex adults and help them navigate the health and social care system, by ensuring they receive adequate support to attend hospital appointments and have access to the benefits and care they are entitled to. At piloting stage, each community team had a dedicated social worker co-located with healthcare professionals. | Multi-professional community care team (EPCT) providing community nursing and therapies for patients aged over 18 and incorporating eight GP clusters. Community teams aimed at improving coordination between nurses, therapists and social workers and were envisaged to play a crucial role in reducing hospital admissions. EPCTs and integrated Care Teams (ICTs) comprise of district nurses (DN), occupational therapists (OT) and Physiotherapists; Locality ICTs also include community matrons. In each locality, a Rapid Response (RR) team was also established as part of the admission avoidance strategy. RR is a nurse-led service that delivers unplanned and urgent care services in the patients home to avoid non-elective hospital admissions. RR team is based within the hospital but managed by community services Trusts | With NHS foundation trusts and local authorities, three East London municipalities came together to form an integrated care programme and achieved pioneer status | Face-to-face; outreach | Care navigators (e.g. social workers in the pilot phase) | The integrated care programme brought together Clinical Commissioning Groups (CCGs), providers (NHS Trusts) and local authorities of the municipalities | Rapid Response (RR) tea, and Discharge to Assess (D2A) teams, and integrated community teams work collaboratively provide holistic care to patients in the community | Funding from NHSE (£20,000 initially, later supplemented with a further £90,000) was given. | NR* |
Cammyet al. 2017 | Yes | A palliative care- and hospice-trained clinical oncology social (POR PCP) worker utilises clinical skills and supports the team in approaching sensitive and challenging end-of-life discussions with clarity and compassion. The social work team member responds to patient and family's feelings as they relate to their past experiences with previous family losses including prior involvement with palliative and hospice care. Interventions may include connection to services to prevent caregiver breakdown, education on signs and symptoms of disease progression, and assessment of high-risk bereavement concerns | Radiation oncology physician expert palliative care, acute care nurse practitioner, registered nurse, and registered dietician | Palliative radiation oncology team was created at the University of Pennsylvania in 2013 | New consults and patients under active treatment are conducted in health settings. Telephone contact with patients is available as many patients transitioned to hospice care or are homebound | Social workers | Palliative teams established bimonthly oncology team rounds, called integrative cancer care rounds. This offered a formal gathering to review current and shared palliative patient cases to enhance communication between multiple palliative specialties | The University of Pennsylvania palliative radiation oncology team includes a radiation oncology physician who completed specialized fellowship training in palliative care, nurse practitioner with advanced certification in acute care, registered nurse, licensed clinical social worker with palliative care and hospice experience, and registered dietician | NR* | Some system integration has been developed. The PRO PCP was created in the electronic medical record (EMR) program |
Chnget al. 2021 | Yes | The links worker programme (LWP) was expected to operate at three levels: patient, practice, and community: at the patient level, practices were to set up referral systems so that GPs and practice nurses could refer patients who they thought would benefit from engagement with community resources to the community link practitioners (CLP) for one-to-one work; at the practice level, CLPs were also expected to act as agents of change promoting the ethos of social prescribing among all staff by, for example, enabling activities to support staff wellbeing, activities to develop shared learning, and awareness about community resources, gathering intelligence about local resources and solving problems through the redeployment of staff; and at the community level, CLPs were expected to build networks and cultivate relationships with local community organisations, develop referral pathways and multiagency resolution of problems, and organise shared learning events to consolidate new and existing community linkages | GP practices and practice nurses providing health | Practices in Glasgow, funded by Scottish Government | Face-to-face | Community Link Practitioners | NR* | Each intervention practice had a full-time salaried CLP appointed, who was employed by a Scottish Government-funded third-sector organisation (the Health and Social Care Alliance Scotland). The CLPs were selected by the programme manager and clinical lead, who also made the final decision on which practice assigning each CLP | Each intervention practice had a full-time salaried CLP appointed, who was employed by a Scottish Government-funded third-sector organisation (the Health and Social Care Alliance Scotland). Intervention practices were also provided with a practice development fund of £35000, around 80% of which was used for creating more time, particularly clinical time for GPs (and the practice nurse in one practice) to have longer consultations with patients. Practices also invested to free-up receptionist time, by, for example, hiring another receptionist or purchasing self-check-in systems | NR* |
Collinset al. 2017 | Yes | The initiative provides low-threshold nursing care services (e.g. health assessments, medication assistance, support, symptom management) and social support and programmes (e.g. recreational therapy outings, karaoke). Residence and day health programme provide counselling services, including art and music therapies, and mental health resources and referrals. Day health programme provides, nutrient-dense meals twice daily, seven days per week, and residence provides clients with regular meals and snacks. Staff provide referrals to supportive and subsidised housing, particularly housing intended for PLHIV (people living with HIV; | The initiative provides highly active antiretroviral therapy (HAART) and retention in HIV care. Integrating supersised injection into the Dr. Peter Centre (DPC) residence and day health programme | The DPC, a Vancouver-based HIV care sersice organization, employ's an integrated sersices model and provides sersices to approximately 425 PLHIV annually | Face to face | Nurses | Adoption of comprehensive model to minimize barriers PLHIV who inject drugs face when accessing care sersices and consults with decision-makers (eg. policymakers, police) to increase awareness of the public health benefits of this approach | NR* | NR* | NR* |
Davenportetal.2021 | Yes | Occupational interventions are aimed at maintaining safety in essential activities of daily living (ADL), falls prevention, moving and handling solutions such as hoist and specialist sling provision or bed mobility solutions and major adaptations such as level access shower, stairlifts, through floor lifts and ramping, specialist seating provision and liaison with local housing services. Interventions can consist of telephone advice, or one or more visits depending on complexity | Rehabilitation or intermediate care service provision (primary care) which are provided by the Trust. | Occupational therapists, plus support practitioners working for the adult social care service covering Wirral local authority were integrated into Wirral Community Health and Care NHS Foundation Trust (WCHC) in 2017 | Face-to-face | Occupational therapists | NR* | NR* | The initiative is funded by NHS Foundation Trust | Patients records are recorded and taken from the adult social care recording system Liquid (https://www.liquidlogic.co.uk/) by a Trust information analyst |
deVriesMcC Unlocket al. 2016 | Yes | The basic interienti on involved the interventionist collaborating with physicians to provide education, guideline-based treatment recommendations, and to monitor adherence and clinical indicators. Key components of the basic intervention were: (1) an individualized program to improve adherence to oral hypoglycemies agents or anti-hyperglycemic agents; and (2) integration of depression treatment with Type 2 Diabetes Mellitus (T2DM) management. Patient prioritized planning (PPP) was introduced. The goal was to identify priorities that were likely to influence adherence to treatment. Biomedical needs as well as financial, social, and emotional needs patients with T2DM and depressive symptoms. Participants received information about local resources (e.g. emergency shelter services, the Department of Public Welfare, disability services, Medicare and Medicaid, social security income) | Physicians services provision aimed at diabetes and depression treatment | Physicians practices in Philadelphia, Pennsylvania | Face-to-face | Interventionists | NR* | NR* | NR* | NR* |
Dohenyetal. 2020 | Yes | The 290 municipalities provide the social care services (ie, home-help including both household and personal care senices) needed by older persons (regions and municipalities are independent, as they both collect taxes to finance most care services) | Primary healthcare (PHC) is the basis of the Swedish healthcare system, where most patients with chronic diseases are treated, and includes home-health care services | IC was initiated as a shared project between Norrlje municipality and Region Stockholm | NR* | Hospital-based care teams | The Norrtlje model was set-up to provide care to the entire population of the municipality. The intersenti on had its base at the hospital and set out to join the efforts of health and social care services, through aligning medical documentation, care planning, rehabilitation, preventative care, home-help, home-health care and PHC services. Care teams were created with specific purposes to facilitate inter-professional group meetings, for training and to improve service delivery. The model facilitated the development of a variety of care paths (eg, dementia, stroke), in addition to the national care plans for certain conditions already established in Sweden | Care teams were created with specific purposes to facilitate inter-professional group meetings, for training and to improve service delivery | A joint health and social care board with politicians from Region Stockholm and Norrtlje municipality was formed, responsible for the financial and organisation administration as well as the purchasing of care services from a jointly owned public company (tax-funded). The Norrtlje Model used a shared approach to policy and financing in order to promote a better integration of resources and care staff, and further, provided a stimulus for the development of a shared information system to facilitate IC | A stimulus for the development of a shared information system to facilitate IC. Shared information systems were reported |
Eastwoodet al. 2020 | Yes | Sustained Nurse Home Visiting services for vulnerable mothers and their infants until 2 years using a tiered approach. Intensive wrap around counselling models for high-risk mothers experiencing interpersonal violence, and with complex mental health and substance use problems Preschool and school-based centre and home visiting interventions to reduce conduct disorder, bullying, depression, and alcohol use | Early intervention and public health approach to interrupting cycles of family disadvantage, poor health and psychological trauma. Use of evidence-informed integrated care methods by service partners, including family case conferencing, and wrap-around care delivery. Providing a supporting structure to general practice providers to care for families that are often seen to be too difficult | Sydney Local Health District implemented an integrated care initiative for disadvantaged families in the Inner West region of Sydney, Australia. The initiative, known as Healthy Homes and Neighbourhoods (HHAN), is designed as a cross-agency care coordination network for disadvantaged families. At the level of service providers, the New South Wales. (NSW) Government, Australia | Face-to-face | HHAN consists of five service-providers: three senior clinical nurse consultants and two senior social workers. Two service-providers are based in the place-based multiagency hub in Redfern, two service-providers are based in the community centre in Riverwood, and one service-provider covers the families enrolled in HHAN who are located between the two areas. All service-providers work independently, however, come together weekly for case reviews, intake meetings, and business meetings | In 2014, collaborative interagency work commenced on an Inner-West Interagency Child Health and Well-being Plan. Following the launch in 2014 of a New South Wales (NSW) Government integrated care initiative, the Healthy Homes Neighbourhoods (HHAN) Integrated Care Initiative was designed | HHAN consists of five service-providers: three senior clinical nurse consultants and two senior social workers. Two service-providers are based in the place-based multiagency hub in Redfern, two service-providers are based in the community centre in Riverwood, and one service-provider covers the families enrolled in HHAN who are located between the two areas. All service-providers work independently, however, come together weekly for case reviews, intake meetings, and business meetings | SLHD provides independent budget for this program. | NR* |
Elstonet al. 2019 | Yes | The Well-being Coordination service uses 12 Co-ordinators employed by 7 key voluntary sector organisations, embedded in local communities across the area. Co-ordinators are based in a variety of settings, including NHS premises. The Co-ordinator works with the individual for up to 12 weeks to enable them to take action to achieve their goals. This includes resilience-focused coaching and practical support and advocacy to navigate and access local health, social and economic services. | GPs, community and social care staff in multidisciplinary meetings, hospital discharge staff (acute and community) | In Torbay and South Devon, the Integrated Care Organisation, a provider organisation, commissioned a SP service from the voluntary sector to be integrated into its five locality hubs, alongside primary care, community and social services | face-to-face; outreach | Co-ordinators (Social Prescribing) | South Devon service commissioned by Torbay and South Devon NHS Foundation Trust is managed by Teignbridge CVS, an umbrella voluntary sector organisation | This study focuses on the South Devon service commissioned by Torbay and South Devon NHS Foundation Trust and managed by Teignbridge CVS, an umbrella voluntary sector organisation | Social prescription service from the voluntary sector to be integrated into its five locality hubs, alongside primary care, community and social services | Data on the use of health and social care services were collated from local IT systems 12 months prior to and after the date of each referral. It included the following services: accident & emergency (A&E) and minor injury units (MIU), in-patient, outpatient, community service (ie, occupational therapy, physiotherapists and nursing) and social service contacts and length of stay (in-patients only) and GP contacts. Contacts outside the clinical commissioning group (CCG), boundary were also included |
Ismailet al.2020 | No | Social interventions lead by a community support worker if social problems were recorded involved advocacy in housing, debt problems, childcare, domestic violence, immigration and/or signposting to employment training. These were integrated into their routine diabetes care by ensuring 3DFD clinics were co-located with the diabetes MDT clinics via joint consultations with the key diabetes healthcare professionals or weekly feedback at the generic diabetes MDT meetings. The 3DFD liaison psychiatrist and/or community worker met the participant in weekly-to-monthly appointments, depending on their needs, for a period of up to 6 months | A multidisciplinary diabetes team MDT), which included a general practitioner (GP), diabetologist, diabetes specialist nurse and dietitian in three settings of increasing severity: primary, intermediate and secondary care for diabetes. Any professional from the diabetes MDT in Lambeth and Southwark could refer adult individuals to 3DFD via a standardized online or paper referral form. Each referral was discussed and triaged at weekly 3DFD team meetings attended by the psychiatrist and community worker and allocated to: the liaison psychiatrist (if the referral indicated pressing safety concerns or presence of multiple psychiatric morbidities) for a diagnostic assessment and initiation and monitoring of psychotropics; assessment for psychological therapy | Research Centre for Mental Health at the South London and Maudsley NHS Foundation Trust and loPPN, King's College London. 3DFD was set in Lambeth and Southwark, London, UK | Face-to-face | The 3DFD team consisted of a full-time consultant liaison psychiatrist and two full-time community support workers from a third sector (or nongovernmental organization), voluntary organization, Thames Reach, that provided social welfare | NR* | The 3DFD team consisted of a full-time consultant liaison psychiatrist and two full-time community support workers from a third sector (or nongovernmental organization), voluntary organization, Thames Reach, that provided social welfare | the NHS London Regional Innovation Fund, Guy's and St Thomas's, King's, and Maudsley Charities and Lambeth and Southwark Clinical Commissioning Groups | NR* |
Janseet al. 2016 | Yes | Primary Care Practices (PCP) is a cooperative of a hospital, a nursing home, the three largest home-care organisations, a mental health organisation, allied health practices and elderly patient-, informal care and volunteer associations. Home-care organisations were important network partners, as they provide various services in the elderly patients homes through small community-based teams consisting of a community nurse, general | GP and case managers. | A local cooperative of PCPs initiated, developed, and implemented the Walcheren Integrated Care Model (WICM) | Face-to-face | Case workers, community nurse, general and specialized nurses and domestic helpers | Organizational administrative integration was achieved through the creation of a geriatric care network, consisting of the PCP cooperative a hospital, a nursing home, the three largest home-care organizations, a mental health organization, | Small community-based teams consisting of a community nurse, general and specialized nurses and domestic helpers | Integrated funding involved an experimental financial module provided by the regional healthcare insurer to reimburse intervention-related costs to participating PCPs | NR* |
and specialised nurses and domestic helpers. Services range from around-the-clock supervision and/or specialized nursing care, home recovery/rehabilitation, home meal services, personal care and domestic assistance | allied health practices and elderly patient-, informal care and volunteer associations. Network partners, governmental social care/welfare organizations and the municipalities formed a steering group that was responsible for the further development and planning of the WICM | |||||||||
Mateo-Abadet al. 2020 | Yes | The CareWell integrated care model has defined a specific pathway for patients with multimorbidity (addition to the usual/primary care). It has several phases: identification of frail older patients, comprehensive baseline assessment, definition of the therapeutic plan, programmed follow-up, patient stabilisation at home, integrated care during hospitalisation and coordinated hospital discharge. The pathway focuses on two main dimensions: l)care coordination and communication between health providers and 2) patient empowerment and home-based care. A patient empowerment program, KronikOn, was defined. The KronikOn targets frail older patients and their carers. | Primary Care professionals, GPs and Primary Care (CP) nurses are responsible for most of the healthcare activities performed at the community and home levels, such as on demand consultation, home visits, drug prescription, patient education, or referral to the specialist or hospital care all recorded via electronic health records (EHR) and e-ρrescriρtion availability and eHealth call centre, staffed by trained nurses available to respond to phone calls from patients. A dedicated consultant can coordinate other specialists during the hospitalization period. A dedicated consultant can coordinate other specialists during the hospitalization period. Discharge is coordinated between the hospital liaison nurse and the PC nurse | The Department of Health of the Government of the Basque Country and the Basque health system, Osakidetza, has deployed a specific strategy to improve the structural integration and care coordination | Follow-up within 24 hours after discharge and monthly telephone calls by the PC nurse to allow early detection of possible deterioration. Messaging between patients and/or carers and healthcare practitioners via the Personal Health Folder was enabled and outreach as needed | A dedicated consultant can coordinate other specialists during the hospitalization period. Discharge is coordinated between the hospital liaison nurse and the PC nurse | Multidisciplinary primary care teams and collaboration among different disciplines in multiple planning activities related activities are central to the integrated approach. Geriatric expertise is easily accessible by close involvement of elderly care physicians and geriatric staff | The multidisciplinary teams include the following profiles: the General Practitioner, the Social Worker, the Specialists, the Nurse Care Manager, and the eHealth Centre. The Nurse Care Manager is responsible not only for the specific case management but also supports the patients in the hospital, emergency department, and during the discharge process. The roles of the Reference Internist and the Hospital Liaison Nurse are reinforced | This was funded by Department of Health of the Government of the Basque Country and the Basque health system, Osakidetza | These are supported by ICT-based platforms, including a Personal Health Folder, which allows the patients to access their clinical information |
Melvinet al. 2019 | Yes | The Open Arms program involves case management, and social support services linkage (transportation, emergency food assistance, housing, and legal service) Case management. The clinical case manager assesses the patients’ medical and psychosocial needs. The manager works with patient navigators to coordinate all referrals internal to and external to Open Arms and facilitates all HΓV and behavioural health care linkage within 24 hours. Referrals to social support services are made on the same day and are based on the patients’ needs. Social support services. The model provides wrap-around sendees in the form of internal and external referral sendees (ie, support groups, transportation, and emergency food assistance; housing, employment sendees, and mental health sendees) | HIV care (primary health care), behavioural health care (mental and substance abuse screening and treatment), and adherence counselling (a pharmacist-led intervention) | The Open Arms Healthcare Centre (Open Arms) is a nonprofit health care organization established in 2013 to provide innovative, holistic, health care sendees to undersened, underinsured, underrepresented populations in Mississippi with emphasis on lesbian, gay, bisexual, transgender, and intersex populations | Face-to-face; telephone | Case managers and patient navigators | NR* | NR* | NR* | Data were collected and stored in Advanced MD, the Open Arms medical record system, and CAREWare (https://hab.hrs a.g ov/program-grants-manag ement/care ware), a free, electronic health and social support sendees information system for Ryan White HIV/AEDS |
Moonet al. 2021 | Yes | Emotional wellness promotores conducted an exploratory session to uncover the priority issues for the participant and identify their most pressing social needs. Thereafter, participants engaged in group sessions and one-on-one sessions with a promotor by using a curriculum based on principles of narrative therapy. Promotores provided a range of interventions, including education (navigating legal, medical, education, penal, or immigration systems), peer support (donations, goal setting, identifying strengths and barriers, moral support, system support), leadership development (advocacy and individual coaching), community building and engagement (group projects, activities, volunteering), addressing barriers to service use (application assistance, childcare, health care access, translation services, transportation arrangements), and referrals to legal, social, and health services. After COVID-19, social needs proliferated and promotores assisted with COVID-19 financial relief, nutrition assistance, and affordable housing support | Health care service provision via Latino Health Access (LHA) services | LHA, a nonprofit public health organization in Santa Ana, California, partners with Latinx communities in Orange County to advance health equity and run culturally appropriate services | Once COVID-19 struck, service delivery changed: group sessions convened via video conferencing, and one-on-one sessions were carried out over the telephone | Emotional Wellness Promotores (incorporating equity in a COVID-19 community mental health intervention in the Latino communities) | There is a strong collaboration between LHA, a non-profit public health organization in Santa Ana, California, and Latinx communities in Orange County. | Promotores are integrated and part of the LHA services, incorporated equity | LHA Emotional Wellness Program receives contributions from the Orange County Community Foundation, the Keith and Judy Swayne Family Foundation, and the Health Care Foundation for Orange County. CARES ACT has provided emergency rent relief in May 2020 (USI.6 million). Cify council approves 2S.6 million via CARES act for rental assistance, childcare, testing, community resources in 2020 and 2021. | NR* |
Moretti et al. 2017 | Yes | Social workers accompanied acute brain injury (ABI) people and their families for six months to conduct a support path, from hospital discharge to home care and social reintegration. The criteria for the identification of families were agreed upon by the project team, with the following requirements being considered essential: high intensity care needed by the person and the family, the need to activate a variety of resources in the Marche Region | Hospital-based care | Centre of Research and Service on Social and Health Integration (CRISS) of Polytechnic University of Marche, The Santo Stefano Rehabilitation Institute, in Porto Potenza Picena, Marche Region, and the Andrea Brain Injury Association of Marche and other voluntary* organizations | Face-to-face | The social workers are implementing the support path, as well as the operators of social and healthcare services and voluntary organizations. This activity favoured a greater understanding of both the needs of people with ABI and their families, as well as those of the organization, the working methods and problems of local services | A technical group, consisting of representatives of the subject partner, defined the objectives of the project and the methods for testing and verification, while the creation of a working group, composed of social workers actuated the support path, enabling the interventions to be monitored | Social workers assisted with the creation of a map of services and resources, collaboration with GPs, collaboration with the health and social services. These actions, while maintaining a character of continuity, take on specific features in each of the three phases. With regard to collaboration between the services, the meetings organized by the social worker during the support path, which were attended by social and healthcare services and the families, favored the use of a shared vision of the situation, the definition of actions to be implemented and mode of link | NR* | NR* |
Murphyet al. 2017 | Yes | The intervention was admission to a purpose-built health and social care day facility to receive services provided there by a multidisciplinary team of health and social care professionals: nurses, doctors, social workers, physiotherapists, and occupational therapists. Depending on the needs identified, the client had access to an individually tailored programme of interventions. These could include assistance with activities of daily living such as personal cleansing, hair care, mobility and elimination, occupational therapy, and physiotherapy as well as other nursing and social work interventions. The interventions provided depended on the client's individual needs, however optimum nutrition was emphasised for all. The unit offered a programme of activities such as music groups, choirs, bands, quizzes, bingo, raffles, shopping project. No specific incentives to attend were offered but in keeping with normal practice, transport was provided | If more specialist referrals were required such as to specialist nurses, dieticians, audiologists, and podiatrists then this was actioned. A general practitioner visited the unit at least once weekly. | Integrated Health and Social Care day unit (IHSCDU) | Face-to-face | Nurses, social workers, and occupational therapists | The integrated care provision was a purpose-built IHSCDU established in 2007. A multidisciplinary team of health and social care professionals who collaboratively. | Nurses, doctors, social workers, physiotherapists and occupational therapists. Referral routes were via individuals themselves, their families or health and social care professionals, such as general practitioners and social workers | NR* | NR* |
Pauleyet al.2016 | A new program has been developed that integrates cluster care and supportive housing models. In the supportive housing model, services and housing are combined in the same location. Integral to this approach is an interdisciplinary care team composed of shelter/alternative housing staff, and a personal support worker (PSW), and health professionals as well as a care coordinator responsible for providing intensive case management. As the supportive housing model gathers people with similar needs into one location, the cluster care model can be easily implemented | A primary care physician, a psychiatrist, a dedicated registered nurse (RN) | NR* | Face-to-face | Interdisciplinary care team composed of a primary care physician, a psychiatrist, shelter/ alternative housing staff, a dedicated registered nurse (RN), and a personal support worker (PSW), as well as a care coordinator | NR* | Both social and health care providers are part of an integral team | NR* | NR* | |
Permanet al. 2021 | Yes | The counsellors carried out a review of the social and biological situation in the patients’ home, following a structured process, evaluating different domains: functionality, nutrition, mobility, pain, cognition, medication reconciliation and adherence evaluation, need for care and supervision, quality of care, and environmental safety. | Medical coordinators (family physicians, internists or geriatricians) were responsible for health care provision | Hospital Italiano de Buenos Aires | Face-to-face, outreach | Health and social care counsellor | NR* | Different professionals (health and social counsellors) were involved to achieve an interdisciplinary team with complementary* skills. Together with medical coordinators (family physicians, internists or geriatricians) who had no assistance role in the programme, discussed each case from a broad perspective, integrating both clinical and social problems | Embedded in hospital funding | NR* |
Pruittet al. 2018 | Yes | HealthConnections represents a new model of medical and social service coordination. Participants with unmet social needs have contacted the call centre-based program to obtain free referrals to a nationwide network of local, community-based public assistance programs. The program matches participant needs to available social services such as transportation, food programs, financial assistance for utilities, education programs, and housing services | Referrals for medical service provision is also available | HealthConnectio ns was developed by WellCare Health Plans, Inc., a managed care organization (MCO) | Phone service provision | HealthConnections employs a team of individuals responsible for identifying, collecting, maintaining, and analysing the database of community-based social service organisations. The call centre is staffed with representatives who have personal experiences with the social service system, Program representatives follow* up with the participants to confirm whether the social services met their social needs | NR* | The program connects individuals with social needs to the appropriate services. | NR* | The MCO programs database contained hundreds of organizations offering more than 60 categories of social services. The program tracks each referral in the tracking database separately |
Sadaranganiet al. 2019 | yes | The Community-Based Health Home (CBHH) model was designed to incorporate Health Home required services (comprehensive care management, care coordination, health promotion, comprehensive transitional care/fol low-up, patient and family support, and referral to community and social support services) using the existing infrastructure of the strength-based Adult Day Health Care (ADHC) model. The registered nurse navigators (RN-Ns) work with the ADHC EDTs (registered nurse, physical therapist, occupational therapist, speech pathologist, social worker, and dietician) in coordination with the physician. The RN-lTs priority is to promptly address emerging crises within a high-risk caseload of patients. The RN-N also supports the physician’s care plan, coordinates with caregivers and other providers, and formulates patient-centred action plans to stabilize and improve participants health. The overall goals of CBHH are to stabilize individuals social, medical, and psychological conditions and reduce unnecessary utilization of health services while improving quality of life and self-care capacity | ADHC professionals (registered nurse, physical therapist, occupational therapist, speech pathologist, social worker, and dietician) provide care for vulnerable, chronically ill adults | ADHCs | Face-to-face | A full-time RN-N manages an average case load of 19 patients, providing an average 2 hours of high-intensity care to each participant on a weekly basis | U.S. health care delivery system, Affordable Care Act in 2010, Medicaid State Plan benefit for states to establish Health Homes under the authority of the Affordable Care Act of 2010, Section 2703 (1945 of the Social Security Act), CBHH model, and the ADHC model | Services are provided through the inclusion of a RN-N within the ADHC IDT (ALE, 2016) that support integration of health and social services. | Existing infrastructure of the strength based ADHC model, which has existed in the United States since the early 1980s | RN-Ns shared clinical data with providers, participated in clinical encounters across health care settings, recognised and intervened with respect to emerging clinical issues, and advocated on patient’s behalf |
Sohanpal et al. 2017 | Yes | The social prescribing service: Patients were referred to a social prescribing coordinator. At the first meeting with the coordinator, the patients discussed their personal circumstances and if possible, a mutually determined well-being action plan was devised. The action plan contained goals for improving patient wellbeing, in some cases this involved referring patients to community organisations and services. If necessary, a volunteer was assigned to help the patient achieve their goals. Volunteers were trained by the social prescribing coordinators to assist in the delivery of the service and provide additional support to clients. Patients could receive up to six sessions with the social prescribing coordinator and as many contacts with the volunteer as required | GPs -community based | In January 2014 the London Borough of City and Hackney Clinical Commissioning Group (CCG) commissioned a pilot project for a social prescribing service in three areas comprising 22 primary care general practices. The aim of the social prescribing service was to improve patient well-being and increase personal self-efficacy shown by a reduction in primary health care resource | Face-to-face | Three areas in the borough were included and were assigned a social prescribing coordinator. The coordinators were trained in social work and employed by a managing third sector (not-for-profit) organisation commissioned to implement the service. Three social prescribing coordinators were appointed and worked in the 22 GP surgeries enrolled. | NR* | GPs referred patients with specific social needs to a social prescribing coordinators | NR* | NR* |
Spoorenberget al. 2019 | Frail people and those with complex care needs received individual support from a case manager. The participant and case manager jointly developed an individual care and support plan which targeted all health-related problems identified during history taking using the Geriatrics. Case managers organised the care and support as decided on in the care and support plan. They monitored changes and navigated the plans delivery. Participants were also invited to follow a self-management support and prevention program that included regular Embrace community meetings, which focused on staying healthy and independent for as long as possible | GP or elderly care physician service provision (with particular focus on multimoibidity) | Dutch Organization for Health Research and Development, University Medical Center Groningen (UMCG), The National Care for the Elderly Program and the managerial netwoik of the Regional Network Northern Netherlands | Face-to-face | Case managers, a district nurse and a social wotker for the participants with complex care needs and participants who are frail | NR* | A multidisciplinar; Elderly Care Team consisting of a general practitioner, a nursing home physician, 31 and 2 case managers, a district nurse and a social worker for the participants with complex care needs and participants who are frail, respectively organized care and support for older adults | NR* | During these visits, case managers took a history using the Geriatrics, which was integrated into the web-based electronic record system of Embrace. Within Embrace, the Geriatrics was used for history taking from older adults who are frail and those with complex care needs receiving individual care and support by a case manager. The clinical infoimation systems will be represented by the Electronic Elderly Record System (EERS), a web-based application built for both clinical and research purposes |
Talbotet al. 2020 | Yes | Adolescent Multi Agency Specialist Service (AMASS) offered three different intervention packages which are leading by a social worker embedded in the service (in collaboration with a multidisciplinary team): home stability to stabilise the family home environment to prevent the adolescent from entering care; foster placement stability to stabilise the foster placement to prevent the adolescent being moved to an alternative placement; and return home to support an adolescent to move from acare setting (e.g. residential setting, secure unit and foster care) back to the care of their family | Use of individually tailored, evidence-informed methods of practice informed by a range of evidence-based approaches (e.g. behavioural parent training, systemic family therapy, cognitive behavioural therapy, motivational intersiewing, etc.) | AMASS service | Face-to-face; outreach | Lead Social Worker | The service was commissioned by the Local Authority. AMASS was jointly managed by a local authority employed Social Care Manager and a National Health Service (NHS) employed Child and Adolescent Mental Health Service Clinical Psychologist, alongside two Senior Social Workers, a specialist Teacher, a Youth Worker and an Assistant Psychologist. | A multi-agency team was co-located within Children Social Care, to which social workers could refer cases with which they wanted support to jointly deliver a social care, mental health and education intervention designed at reducing edge of care risk | The service was commissioned by the Local Authority to reduce the number of young people coming into care compared with previous years | NR* |
Terracdanoet al. 2021 | Yes | There is a network of volunteers (neighbours) and professionals (GPs, the pharmacist) around frail older adults. The evaluation is followed by the intersentions that are identified in collaboration with social workers. Within the program, social workers draft individualised care plan, coordinate the intervention to implement it at the older population, and taking care of their specific social needs. Interventions reflect the specific needs of the elderly both in the social and health fields. The most frequent intersenti on is changing the environment to prevent home falls; socialisation; medication review; education to have a correct diet; support to search for a paid assistant; social support to the household; home care; and emotional and psychological support | GPs and pharmacy service provision | Lazio Regional Health and Social System, and the University of Tor | Telephone calls, home visits for organisation of dedicated activities | Community nurses (ON) | NR* | The interventions performed by community nurses in the Long Live the Elderly (LLE-CN) group were carried in collaboration professional integration among nurses, social workers, psychologist, and GP | NR* | NR* |
Tonget al. 2020 | Yes | Coordinated care Social care providers of the older people’s centres were invited to observe the assessment and caring planning sessions, after which the nurse or the health worker liaised with the social care providers on the status/conditions of the participant so that they could follow the participant throughout to ensure that they receive continued support or care. The report for each participant and the resource kit were provided to social care providers for reference | An integrated intervention consisting of in-depth assessment, personalised care plans and coordinated care: individual interviews were conducted to identify problems or needs, using an electronic questionnaire. Common geriatric syndromes have been considered, which included yes/no questions to the following domains (chewing difficulties, vision impairment, hearing impairment, sarcopenia, memory complaints, self-rated health, psychological well-being, incontinence, instrumental activities of daily living impairment and polypharmacy), followed by in-depth assessment and checking of prescribed medications. | This initiative is part of the Jockey Club Community eHealth Care Project commenced since 2016 for Chinese people aged 60 years or older who are members of older people’s community centres across 18 districts of Hong | Face-to-face | The nurse and the health worker | NR* | The nurse and the health worker | NR* | NR* |
VanDijket al. 2016 | Yes | As part of integrated neighbourhood approach (INA) community workers had health and social care backgrounds. Community workers visited older people at home and mapped their social and physical needs and capabilities with respect to factors such as housing, mobility issues, and social activities, through phased interviews. Together with older people, they sought appropriate solutions to identified problems or needs and composed individualised support plans. Community workers thus served as liaisons at the personal (supporting and monitoring older people), professional (seeking a multidisciplinary approach to support), and community (establishing a well-functioning network and engaging informal support givers) levels | Not part of the INA program | Rotterdam municipality, local health and social care organizations, Erasmus University Rotterdam, the University of Applied Sciences, and Geriatric Network Rotterdam initiated an INA for community-dwelling older people | Face-to-face; outreach | Community workers had health and social care backgrounds | INA combines components found to be effective for integrated care and support provision, the use of multidisciplinary and outreach teams, and preventive home visits | NR* | the National Care for the Elderly Programme, was launched in 2008 and funded by the Netherlands Organization for Health Research and Development | NR* |
Vestjenset al. 2019 | Yes | Community-dwelling older patients registered at the GP practices are screened for frailty using the Tilburg Frailty Indicator (TFI) during a home visit by the practice nurse, homecare nurse or geriatric nurse. The assessment comprised of physical, psychological, and social domains. Problems and needs are reported in multiple domains according to the SFSPC-model, i.e., somatic (e.g., pain, fall risk), functional (e.g., limitations in activities of daily living like problems with eating or household activities), social (e.g., social network), psychological (e.g., fear, coping, depression), and communication (e.g., visual or hearing impairments). Outcomes of this are reported and discussed with the GPs and elderly care physicians. The care plan is then tailored to the personal needs and wishes. Follow-up of older patients is arranged by a multidisciplinary team of (healthcare) professionals and an appointed case manager, who coordinates and evaluates the process, and provides support in goal setting and self-management | Primary health provision by GP practices and led by GPs | Finding and Follow-up of Frail older persons (FFF) approach, which aims to maintain or improve older people’s well-being and is implemented by part of the Dutch general practitioners (GPs) Located in the western part of North Brabant Province, the Netherlands | Face-to-face; outreach | Practice nurse, homecare nurse or geriatric nurse | Multidisciplinary primary care teams and collaboration among different disciplines in multiple FFF-related activities are central to the FFF approach. Geriatric expertise is easily accessible by close involvement of elderly care physicians and geriatric nurses. Older persons (healthcare) needs are discussed in multidisciplinary consultation at least once a year. Individualized care plans include reported problems and (healthcare) needs, tailored (self-management) interventions, plans for multidisciplinary follow-up and evaluation | Multidisciplinary teams are integrated | NR* | NR* |
Whiteet al. 2021 | Yes | Includes liaison with or referral to inpatient and community mental health services, family sessions, allied health including dietician and exercise physiology, other specialist medical services, private psychiatry, psychology and GP services; sexual health, forensic, domestic violence services and social support agencies including financial, vocational, educational, and housing. The service is to provide intensive, integrated, wrap around care across mental health, medical, social, educational and occupational domains, for up to 12 months | Psychologists, general practitioners, social supports, group programmes, specialist, hospital services and after-hours acute care | Headspace, established in 2006 and funded by the Australian Government to provide accessible, youth-friendly, integrated primary care services for early intervention to young people aged 12 years | Face-to-face | The service is to provide intensive, integrated, wrap around care across mental health, medical, social, educational and occupational domains, for up to 12 months, headspace Early Intervention Teams (hEIT) has access to services of headspace and Sydney Local Health District (SLHD) such as psychologists, general practitioners, social supports, group programmes, specialist, hospital services and after-hours acute care. Further details of the model of care of hEIT, staffing and clinician experience, has been published (Nash et al., 2021) | To address these service gaps, new models of sendee were funded by the Australian government through the Primary Health Networks (PHNs) across Australia. Two (hEITs) in Sydney were supported by this funding commencing in 2017. hEIT is a product of interagency collaboration, sitting physically within the youth friendly headspace offices, yet their clinical governance and employment rests with SLHD, while funding is from the Australian Government via the local PHN, and development support comes from Orygen, National Centre of Excellence in Youth Mental Health | hEIT is co-located within the youth friendly clinical spaces of headspace, while clinical governance and staff employment rests with SLHD, an organization that serves a population of 640000 in metropolitan Sydney | To address these sendee gaps, new models of service were funded by the Australian government through the PHNs across Australia. Two hEITs in Sydney were supported by this funding commencing in 2017 | EMRs and systems are in place (SLHD) sendee |
Wong 2020et al. | Yes | Tins is a three-month health-social partnership program. Nurse Case Manager (NCM), functioning as the leader of health-social care team, conducted the initial assessment in the first home visit to identify the clients’ health and social problems within one week of discharge. Community workers, supervised by both the nurse case manager and social worker, provided telephone follow-up and subsequent home visits to monitor the clients progress and provide support when necessary. According to the problems identified, the NCM provided intersentions in accordance with the Omaha System scheme, which included health teaching, guidance and counselling, treatment and procedures, case management and surveillance. The NCM also coordinated care across a range of settings, from the home to the community centre or hospital when necessary | After each client was admitted to the emergency medical ward EMW, an advanced practice nurse (APN) from a hospital discharge team visited them to familiarize him/herself with their condition and prepare a discharge plan. A face-to-face or telephone call handover between the APN and the project nurse case manager (NCM) was performed before the client was discharged. The past and current medical conditions, medical and nursing management, and follow-up appointments were discussed | The community-based health-social partnership (CHSP) program linked to EMW from Queen Elizabeth Hospital, and Hong Kong Hospital Authority, Hong | Face-to-face; outreach and calls for follow-up | A case manager ensures that the support for individual clients in enhancing self-care was comprehensive and property coordinated. The nurse, backed up by a multidisciplinary team, assumed the role of case manager in the program, and home visits and telephone calls were the two approaches to care delivery performed by community workers | Efforts were directed at building a community-based intervention with a health-social partnership to ensure that system resources and collaboration among stakeholders could be activated to provide support to individuals when needed | There was a case manager to ensure that the support for individual clients in enhancing self-care was comprehensive and property coordinated. The nurse, backed up by a multidisciplinary team, assumed the role of case manager in the program, and home visits and telephone calls were the two approaches to care delivery's. Interdisciplinary case conferences were held regularly between the NCM and social workers, with the involvement of the APN if appropriate. During the conference, the health-social team members communicated each other’s role in managing the case, which increased understanding and collaboration in the process. In addition, events such as the progress and concerns of clients, and suggestions for further actions, modifications, or adjustment of interventions were reviewed | NR* | NR* |
Zarnegaret al. 2017 | Yes | Nonmedical interventions consist of artistic, musical and horticultural activities, visits and outings. The group activities have a strong social element. Breakthroughs arise from imaginative listening, sharing and exploring new ideas particularly when they come from patients: their suggestions for social and work activities, for example the choir, have helped shape the service. Homework, for example practising movement exercises or dressing differently, hands over some shared responsibility to the patient as well as enhancing the effect of the therapy. Some participants are supported in their applications for disability benefits for example help with filling out statutory forms and offered personal representation at Department of Work and Pensions (DWP) or equivalent medical examinations and appeal tribunals. They are encouraged to design realistic return-to-work schedules in keeping with their individual aspirations | All treatments and interventions have a self-management focus and are delivered by a team of a doctor, GP with special interest (GPwSI) in pain management and two therapists. Medical and nonmedical aspects of treatment run as parallel, complementary interventions. Two anthroposophie therapies (9), rhythmical massage and eurythmy (gentle movement) are delivered individually in blocks of 7 -8 weekly sessions. They aim to reduce the burden of symptoms (mainly pain, sleep disturbance, fatigue, anxiety and depression) and to restore energy. The confidence and motivation required for self-management is thereby facilitated. The intensity of the interventions is graded according to patients physical and psychological condition as well as capacity and their needs. As symptoms improve the rationalisation of repeat medication, particularly analgesics and psychotropics, becomes possible | The intervention has been developed and delivered by a charity, Kairos Rehabilitation Trust (KRT), alongside a community pain management clinic, the V anbrugh Community Pain Clinic (VCPMC) in Southeast London | Face-to-face; outreach | Delivered by a team of a doctor, GP with special interest (GPwSI) in pain management and two therapists. Medical and nonmedical aspects of treatment run as parallel, complementary intersentions. Two anthroposophie therapies (9), rhythmical massage and eurythmy (gentle movement) are delivered individually in blocks of 7-8 weekly sessions. They aim to reduce the burden of symptoms (mainly pain, sleep disturbance, fatigue, anxiety and depression) and to restore energy | Community based rehabilitation and social intervention programme which employs the components of the Kings Fund House of Care model. The intervention has been developed and delivered by a charity, Kairos Rehabilitation Trust (KRT), alongside a community pain management clinic, the V anbrugh Community Pain Clinic (VCPMC) in Southeast London | NR* | NR* | NR* |
